Article Text

Statistics from Altmetric.com
Description
Extramedullary haematopoiesis (EMH) is the formation of cellular components of blood, occurring outside of the bone marrow. This is a result of cytokine induction for increased cell production and a greater availability of pluripotent stem cells. While EMH is physiological during fetal development, pathogenic EMH can emanate when physiological haematopoiesis in the bone marrow is ineffective and haematopoietic stem cells migrate to other tissues, as is often seen in disorders of the haematopoietic system, such as thalassemia and myelofibrosis. It has been primarily reported in patients with β-thalassemia intermedia and haemoglobin E-beta thalassemia.1 The spleen and the liver are the most common primary sites for EMH. However, other organs such as lymph nodes, cardiac muscle, mediastinum, lung, breast, kidneys, adrenal glands, thyroid, skin and GIT may also be involved. The diagnosis is almost always histopathological. EMH in the adrenal glands should be considered as a differential diagnosis in patients with haematological disorders who have adrenal gland masses, in order to prevent any potentially unnecessary or inappropriate therapy.2 3
We report the case of a 36-year-old man who had been known to have β-thalassemia intermedia and presented to the clinic for the evaluation of recent onset bilateral pedal oedema. Clinical examination revealed no other findings. He had undergone splenectomy in the past, secondary to multiple blood transfusions. He was also known to have hypertension, for which he had been taking antihypertensive medication. Family history was insignificant. The blood picture showed anaemia and other cell lines within normal limits. Ultrasonography of the abdomen revealed bilateral incidental adrenal masses. CT of the abdomen revealed bilateral adrenal masses with an approximate size of 7 cm (figure 1).

A CT scan of the abdomen showing well-defined, bilateral and non-enhancing adrenal masses approximately 7 cm in size (indicated with arrows).
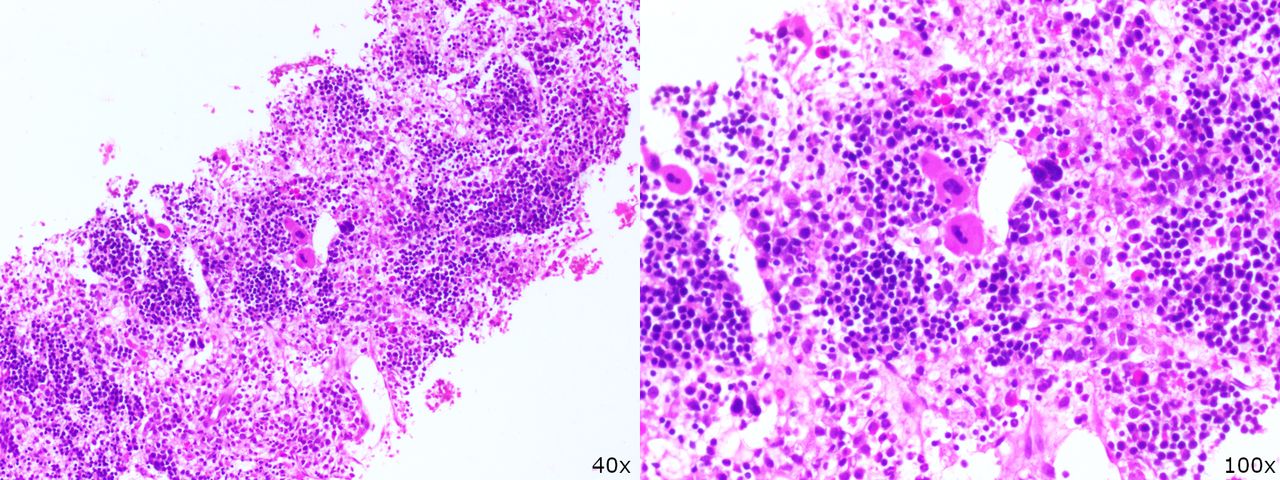
In view of the bilateral adrenal masses, the differential diagnosis considered were tuberculosis, histoplasmosis, lymphoma and the possibility of adrenal extramedullary erythropoiesis. The 08:00 h serum cortisol was within normal limits and biochemical investigations were not suggestive of a functioning adrenal adenoma. For confirmation of the diagnosis, the patient underwent a CT-guided biopsy of the right adrenal mass. Histopathology was suggestive of EMH, showing fibrocollagenous tissue replaced by haematopoietic elements with mature erythroids, myeloids and megakaryocytes, with no granulomas or adrenal tissue in the biopsied section (figure 2). The patient was reassured and was advised for regular follow-up.

{kind=link}
{kind=link}
Histopathology showing trilineage haematopoietic elements with mature erythroids, myeloids and megakaryocytes.
Learning points
It is imperative to consider extramedullary haematopoiesis when adrenal enlargement is seen in patients with haematological disorders, such as thalassemia.
The patient must be adequately evaluated to rule out a functioning adrenal tumour.
A biopsy and subsequent histopathological evaluation are obligatory for confirming the diagnosis.
Footnotes
Contributors MEK composed the manuscript. FKJ, ES and NT provided critical review and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.