Article Text

Statistics from Altmetric.com
Description
A 68-year-old man, with a history of hypertension and smoking, had undergone a total pancreatectomy due to pancreatic cancer, without major complications.
One month after the operation, prior to adjuvant chemotherapy, the patient was admitted to the local hospital with fever (39.2°C) and abdominal pain (Visual Analog Scale (VAS): 5). Laboratory testing showed a C-reactive protein of 68 mg/L and the leucocyte count was 24.9×109/L. The patient was started on intravenous piperacillin–tazobactam and metronidazole. An acute CT of the abdomen revealed a hyperdense area in the sixth liver segment, suspicious of an abscess. Within 6 hours of arrival, the condition of the patient deteriorated rapidly, and he was transferred to the local intensive care unit (ICU) with severe septic shock (quick Sequential Organ Failure Asessment score (qSOFA-score): 3), acute anaemia (haemoglobin 3.7 mmol/L) and acute renal and hepatic failure. Following initial stabilisation, a CT angiography was performed which showed gas formation in the previous hyperdense area (figure 1). The blood culture taken on arrival showed growth with Clostridium perfringens and a small number of Klebsiella variicola. The patient was transferred to the ICU of our hospital and meropenem and ciprofloxacin was added to the antibiotic treatment. An ultrasonically guided drain was placed in the abscess within 45 min of arrival (figure 2). The abscess was drained for air and 400 mL pus. Subsequent cultures from the abscess confirmed the blood culture with growth of C. perfringens and K. variicola. Hereafter, the patient stayed in the ICU for 9 days undergoing hyperbaric oxygen treatment and continuous renal replacement therapy. Most of the blood samples were later withdrawn due to spectrophotometric interference caused by disseminated intravascular coagulation (DIC). The patient was treated for an additional 12 days before being discharged to the local hospital, where he continued intermittent dialysis treatments.

CT 24 hours after hospitalisation showing gas formation in the liver abscess.
{kind=link}
{kind=link}
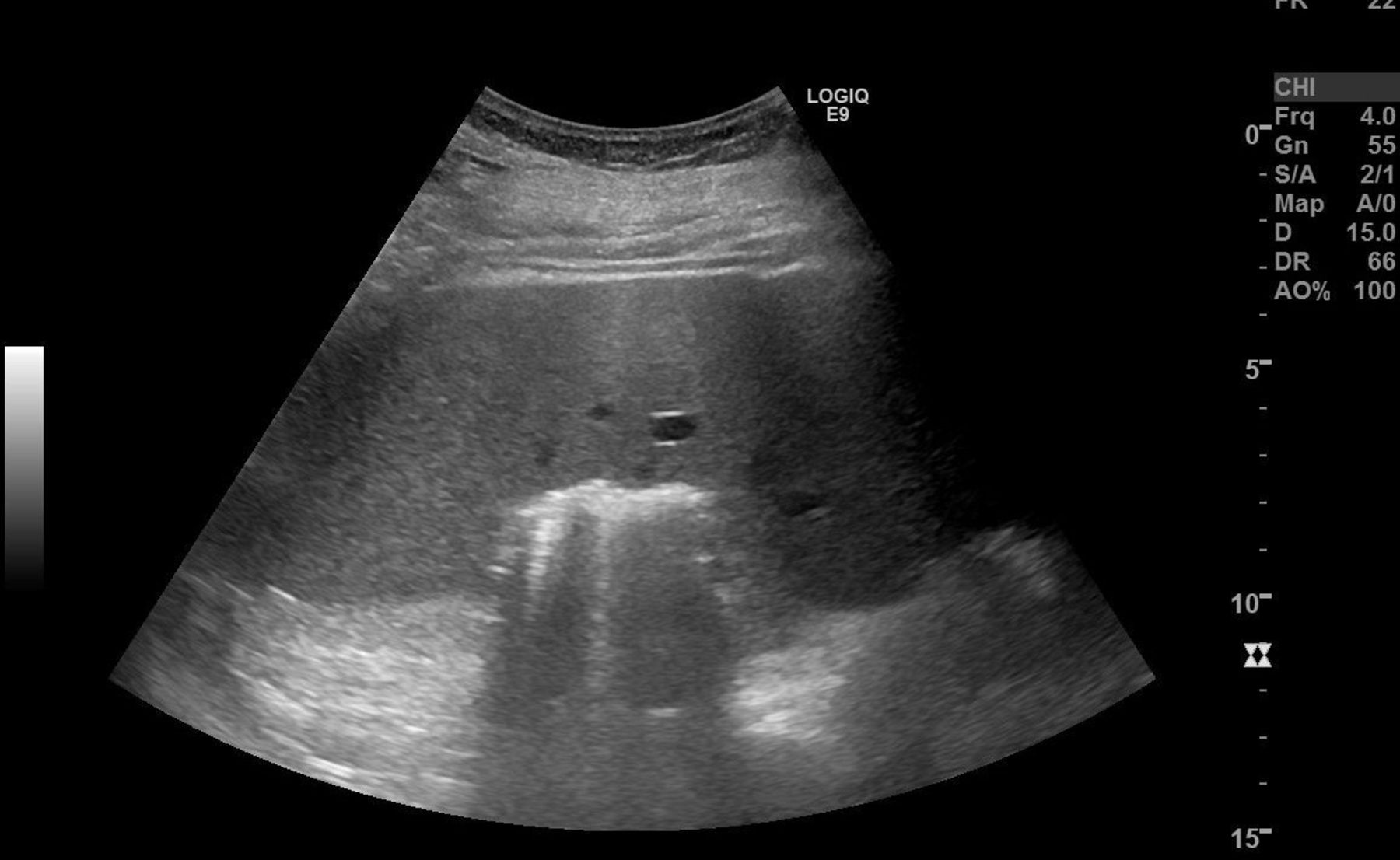
Ultrasound showing liver abscess containing gas and pus. A drain was subsequently placed ultrasound-guided in the abscess cavity.
C. perfringens is the bacteria known to cause gas gangrene, a dangerous skin infection with rapid toxin-mediated tissue gas development followed by necrosis.1 It is an anaerobic Gram-positive rod-shaped bacterium found naturally in dirt samples and in the intestinal tract of humans.
K. variicola is a relatively newly discovered bacterium first described in 2004.2 It is a Gram-negative, non-motile, rod-shaped bacterium found in different plants.2 Due to its new discovery and close resemblance to Klebsiella pneumonia, it is often misclassified as K. pneumonia.3 Being non-motile the bacteria is extremely rare in liver abscesses. To our knowledge, this is the first described case.
Total pancreatectomy is a specialised procedure where the entire pancreas, spleen, duodenum, gall bladder and common hepatic duct are removed, and reconstruction with a hepaticojejunostomy and a gastrojejunal anastomosis is performed. Manifest malnutrition requiring enzyme supplements and insulin-dependent diabetes mellitus is a certain outcome. In this case, a robot-assisted distal pancreatectomy was intended and performed, intraoperative frozen section pathology from the resected surface returned with adenocarcinoma twice. Hence, the procedure was converted to an open surgery total pancreatectomy. Common complications of a total pancreatectomy include haemorrhage, leakage from the hepaticojejunostomy and postoperative infection.
Liver abscess with C. perfringens is a very rare but very severe complication, which has only been reported in a very limited number of cases.1 4 5 The condition was associated with a 70% risk of death.6 Interestingly, the abscesses usually present after infection or surgery involving the bile system.5 Known risk factors are diabetes, cancer immunosuppression or a combination. Once the alpha-toxin has been released septic shock and DIC evolve extremely fast. Time-to-intervention is consistently an important factor in the surviving cases.
The use of bactericide antibiotic might inadvertently cause the release of the toxin from inside the bacteria. Treatment with toxin-antidote has been suggested, but has not been properly tested in humans for this indication.7
Learning points
Liver abscess caused by Clostridium perfringens is a rare but very serious complication to infection and surgery involving the bile system that causes severe sepsis, haemolysis and multiorgan failure.
Rapid evacuation of the abscess and treatment of complications to septic shock seem to be essential factors in patient outcome.
Treatment with antitoxin can be considered, bacteriostatic treatment may theoretically be preferred to bactericide antibiotic.
Footnotes
Contributors SSD, MT and LP had the idea of the study. SSD prepared the manuscript. SSD, MT, T-LL and LP critically revised the manuscript. All authors accepted the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.