Article Text

Abstract
Mycotic aneurysms can pose a diagnostic dilemma due to their variable presentations. We present a case of a 93-year-old man initially presenting with fevers, intermittent chest pain and normocytic anaemia refractory to repeated blood transfusions. He received intravenous ceftriaxone as Escherichia coli grew in his blood cultures. His chest X-ray showed a widened mediastinum. A subsequent CT of the chest discovered a mycotic aneurysm at the descending thoracic aorta. He had a good outcome and was thriving after 1 year post endovascular repair.
- infectious diseases
- vascular surgery
- urinary tract infections
Statistics from Altmetric.com
Background
A mycotic aneurysm occurs when a new aneurysm is formed by infection of a native artery or when an existing aneurysm becomes infected.1 This condition is associated with high mortality and morbidity with high incidence of rupture.2 It can cause a range of symptoms from being asymptomatic to chest pain, abdominal pain, dysphagia, dysphonia and severe bleeding and shock in a ruptured aneurysm.1 Mycotic aneurysms account for 2.6% of all aortic aneurysms with the least likelihood of occurring at the thoracic aorta.1 Arterial injury, arterial luminal defect such as atherosclerotic plaque or ulceration,2 preceding infection,3 compromised immunity, diabetes, alcohol dependence, malignancy and advanced age are predisposing factors of mycotic aneurysms.1
Mycotic aneurysms should be suspected in elderly patients with arterial atherosclerosis, particularly in cases where the source of infection is unclear.1 4 Escherichia coli bacteraemia is frequently encountered in adult inpatient settings and is usually related to urinary tract infections or biliary sepsis.4 Mycotic aneurysms due to E. coli can occur rarely.1
We report a case of E. coli mycotic aneurysm associated with E. coli urosepsis in an elderly man with a background of chronic lymphocytic leukaemia. This case demonstrates the difficulty in making a diagnosis due to the wide differentials and range of symptoms and that prompt diagnosis that enables prompt medical and surgical interventions is life saving.
Case presentation
This case involves a 93-year-old man who is living at home fairly independently. He presented with intermittent chest pain and dry cough starting four days prior associated with subjective fevers and vomiting. He had no lower urinary tract symptoms. On arrival, he was noted to be febrile at 39.7°C. Other vital signs were normal. This is on a background of a low-grade chronic lymphocytic leukaemia treated with ibrutinib.
He had normocytic anaemia (haemoglobin: 77 g/L) and mildly raised total white cell count (9.40×109/L) with predominant neutrophilia (8.46×109/L). His C reactive protein (CRP) was 170 mg/L. Serial troponin levels were normal. His chest X-ray (CXR) done on admission showed a widened mediastinum, which was slightly dissimilar to his previous CXR on close inspection (figure 1). His admission ECGs showed sinus rhythm with left axis deviation but no ischaemic ST changes.

Chest X-ray (CXR) done 6 months prior to admission (left). Patient presented with non-productive cough at the time. Early consolidation in the right middle lobe was seen. CXR done on admission (middle). There was prominence of the aortic arch, coarsening of the bronchopulmonary markings bilaterally consistent with bronchiectasis and a small right pleural effusion. Follow-up CXR done on the third day of admission was not convincing of a new consolidation, but there was subtle expansion in the aortic arch (right).
There was no clinical evidence of active bleeding, but his haemoglobin count dropped marginally to 72 g/L one day after presentation. He received three units of packed red blood cells and his haemoglobin improved to 93 g/L. This started to downtrend the next day to 76 g/L and he received another unit of packed red blood cells.
This patient was initially treated empirically for a community-acquired pneumonia with one dose of intravenous benzylpenicillin 1.2 g and oral doxycycline 100 mg. He was then commenced on regular intravenous ceftriaxone 1 g daily. Due to persistent fevers and growth of gram-negative bacilli in the patient’s blood cultures, the ceftriaxone dose was increased to 2 g daily the next day. Antimicrobial cover was broadened on the third day by switching to intravenous piperacillin/tazobactam 4/0.5 g while awaiting sensitivities. A CT of the chest (figure 2) was performed on the fourth day of admission.
{kind=link}
{kind=link}
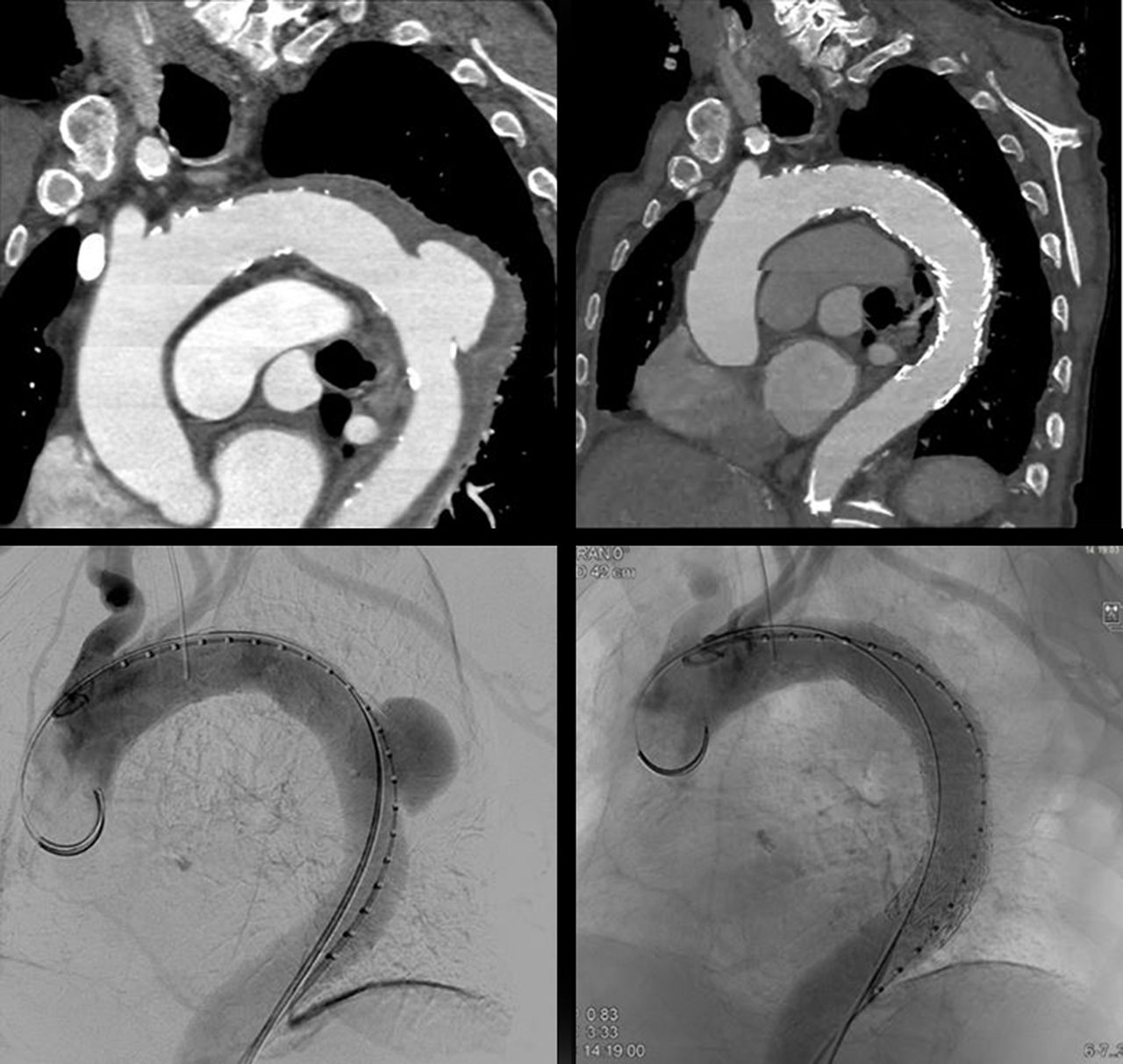
CT of the chest done on day 4 of admission showed a large outpouching seen arising from the posterior aspect of the descending aorta measuring 36×22 mm with intramural haematoma (top left). CT angiogram of the thoracic aorta showing satisfactory appearance after thoracic endovascular aneurysm repair (TEVAR) with resolution of the aortic aneurysm (top right). Direct intensification image before TEVAR (bottom left) and immediately after TEVAR (bottom right).
Investigations
On arrival to hospital, the patient’s septic work-up included bloods, urine, nasal pharyngeal viral swabs and a CXR (figure 1). His bedside random bladder scan showed 135 mL.
His blood film was reactive and the red cells showed moderate rouleaux. Otherwise, his haematinics screen, haemolysis screen and coagulation profile were unremarkable.
Although there was no prior history of urinary tract infection, due to gram-negative bacilli grown in the blood and urine cultures, a urinary tract CT was performed on the second day. It did not demonstrate hydronephrosis, significant renal calculi or a distended bladder.
A CT of the chest (figure 2) was performed due to ongoing chest pains, fevers, new pleural rub on auscultation and subtle evolving mediastinal changes on repeat CXR. It demonstrated an acute aortic syndrome with a large penetrating ulcer arising from the proximal descending thoracic aorta with retrograde and antegrade extension of intramural haematoma along the distal aortic arch and the descending thoracic aorta.
Differential diagnosis
The first CXR finding of a widened mediastinum was noted on presentation to hospital. However, the initial working diagnoses of community-acquired pneumonia contributing to pleuritic chest pain and anaemia secondary to chronic lymphocytic leukaemia were considered to adequately account for his presenting signs and symptoms.
He was subsequently thought to have concurrent urosepsis when gram-negative bacilli were grown in both his urine and all four initial blood culture bottles. They were then shown to be E. coli sensitive to amoxicillin and ceftriaxone.
Unfortunately, his chest pains recurred and his haemoglobin dropped significantly despite receiving blood transfusions the day before. Hence, upper gastrointestinal bleeding was considered. The underlying aetiology was initially under appreciated due to vague complains in the setting of worsening confusion from his delirium.
After the CT of the chest was performed, it was realised that a mycotic aneurysm was the unifying diagnosis.
Treatment
The patient underwent a successful thoracic endovascular aneurysm repair on the fifth day of admission at a tertiary hospital (figure 2). He received intravenous ceftriaxone 2 g daily for 6 weeks in total. This was administered via a peripherally inserted central catheter when he was discharged. Immediately after completing the intravenous ceftriaxone course, the patient was commenced on lifelong oral amoxicillin given his graft insertion whilst actively infected.
Outcome and follow-up
The patient was discharged home 15 days after his operation. His repeat CT angiogram showed improvement in the aortic contour diameter (figure 2). Follow-up reviews in the vascular clinic and in the infectious diseases’ clinic were very satisfactory. His CRP downtrended steadily to 17 mg/L after 9 months of treatment and eventually normalised at 17 months.
Discussion
The majority of mycotic aneurysms are caused by gram-positive bacteria such as Staphylococcus species, Enterococcus species and Streptococcus pneumoniae. Other common pathogens include non-typhoidal Salmonella species. E. coli is considered a rare cause of this condition alongside with Haemophilus species, anaerobes and mycobacteria.1 5
Four cases of E. coli mycotic aneurysms have been reported. Two cases reported non-aortic mycotic aneurysms in the subclavian and internal carotid arteries.4 Multiresistant E. coli was cultured in three cases. Diagnoses were delayed in three cases and only two cases survived. The reported case without diagnostic delay involved an inpatient awaiting type 3a dissecting aneurysm repair. This patient experienced low-grade fevers for 2 weeks, which escalated while awaiting surgery. An extended spectrum beta-lactamase producing E. coli was grown in the blood culture and there was an acute expansion of the aneurysm on repeat CT.6 All three reported cases which had delayed diagnoses involved persistent fevers despite at least 2 weeks of antibiotics treatment.1 4
An infected aneurysm occurs when the intima layer becomes diseased and bacteria then passes through into the deeper layers of the arterial wall. The bacteria proliferate and suppurate causing localised perforation and at times, a pseudoaneurysm forms as the wall degenerates. Atherosclerosis has been linked with the formation of mycotic aneurysm and hence, the aorta is commonly affected. However, mycotic aneurysms can also occur despite the absence of significant atherosclerosis.3
In this case, it is not determined if our patient had a pre-existing aneurysm which became infected or if his aneurysm was caused by the E. coli infection. There is a possibility that he may have had an aneurysm prior given the findings of a widened mediastinum on his CXR from 6 months before admission and had not been previously investigated. However, the management of his condition would have remained unchanged either way.
The recommended initial medical treatment in Australia before blood culture and sensitivity results are available is intravenous vancomycin and ceftriaxone 2 g daily.5 With medical treatment alone, the survival rate is roughly 10%. A combination of prompt medical therapy and vascular surgery can lead to survival rates of about 62%.1 Other studies report mortality rates of infected abdominal aortic aneurysms to be between 23% and 31%.2 Hence, managing mycotic aneurysms require a multidisciplinary approach, including the infectious diseases team, the vascular team and radiology.
Patient’s perspective
I am lucky to be alive … I feel great (1 year after surgery) and I feel like I did not even have surgery.
Patient’s next of kin’s perspective
I remember being called in by you and chatting to me and dad about what was happening and what was going to happen, the surgery. All I could think of at first was how are we going to get there (the tertiary hospital) and what I needed to do next. I do not think dad really understood what was going on. It took a bit of explaining and time before dad decided to go ahead with surgery.
Things were going well after the surgery. I was mainly worried about complications but felt better after speaking with the surgeon. After surgery, dad became aggressive and was not talking sense while he was in intensive care.
It was a few days before he was back to normal after the surgery. I am glad everything went well.
Learning points
Escherichia coli bacteraemia in elderly patients with multiple comorbidities may not necessarily be solely due to urinary tract or intra-abdominal infections.
Thoracic mycotic aneurysms should be considered in the setting of widened mediastinum on chest X-ray (CXR), respiratory symptoms like pleuritic chest pain and dry cough, persistent fevers and positive blood cultures.
In such settings, prompt CT imaging to better characterise a prominent aortic arch when seen on CXR is highly recommended.
Prompt diagnosis of mycotic aneurysm that enables prompt medical and surgical interventions is life saving.
Footnotes
Contributors ZWW formulated the idea for the case report, performed literature search and wrote the manuscript. KO provided comments to the initial draft and assisted with copyediting. All authors contributed to, made revisions and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.