Article Text

Statistics from Altmetric.com
Description
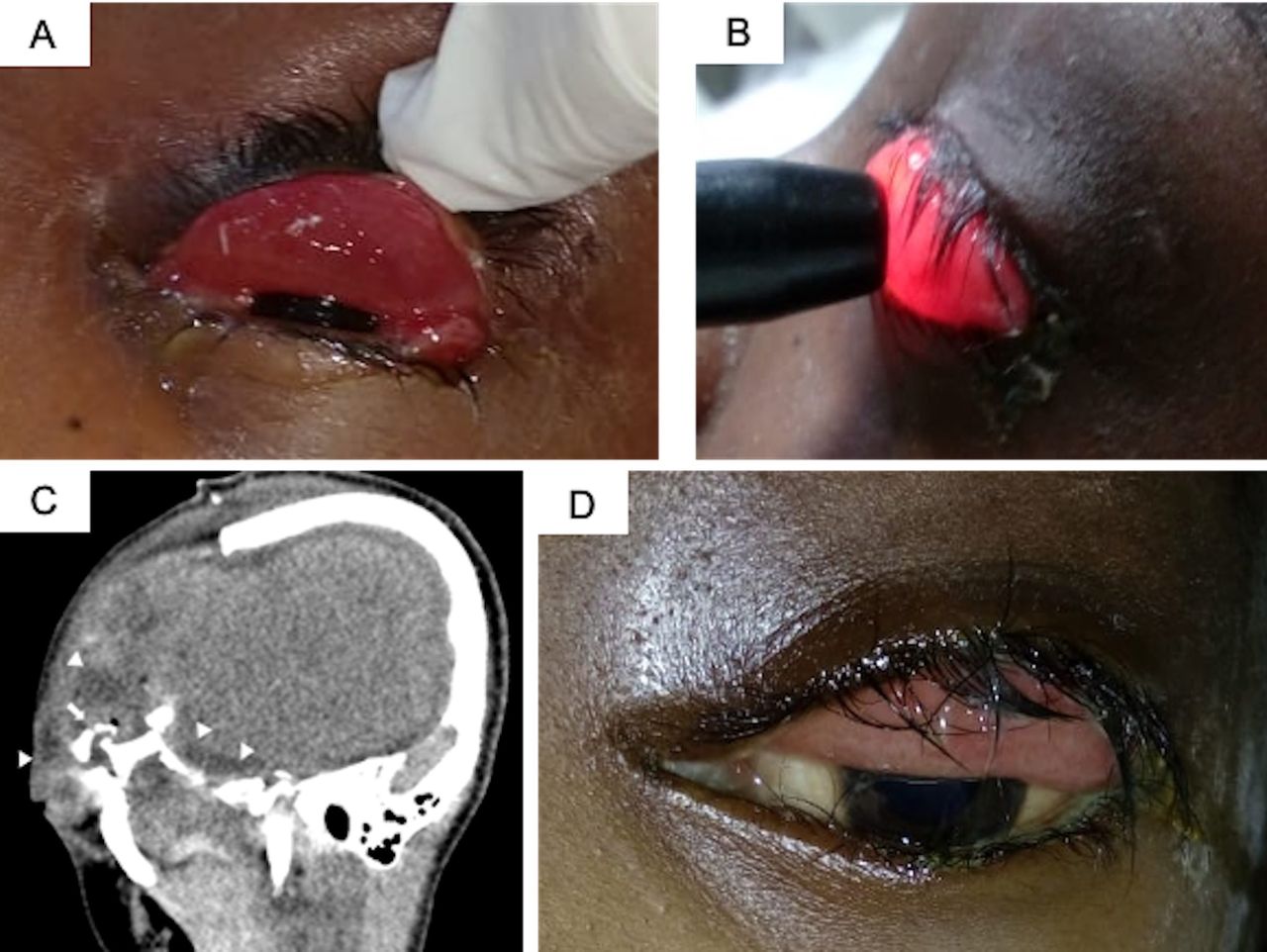
A 13-year-old girl was brought in an unconscious state to the emergency department after having suffered from polytrauma in a road traffic accident. Her Glasgow Coma Scale was E1VTM4. She had undergone emergency craniotomy for drainage of intracerebral haemorrhage. An ophthalmology consult was requested for upper lid swelling with chemosis (figure 1A). On detailed evaluation, the patient was noted to have a transilluminant swelling of the left eye upper lid with forniceal conjunctival prolapse (figure 1B). The bulbar conjunctiva appeared healthy without any chemosis or subconjunctival haemorrhage. The eyeball was intact though the pupillary reactions were bilaterally sluggish. CT scans revealed a comminuted fracture of superolateral wall of the left orbit with swelling of left upper lid with fluid accumulation (figure 1C). A diagnosis of a post traumatic left upper eyelid blepharocele was established.
{kind=link}
(A) Upper eyelid chemosis following severe head trauma; (B) bedside evaluation revealed a positive transillumination test; (C) oblique sagittal image reconstruction of CT scan of the head shows comminuted fracture of superolateral wall of the left orbit (arrow) with swelling of left upper lid with fluid accumulation of cerebrospinal fluid density (arrow heads) and (D) persistent chemosis of the upper eyelid at 10 weeks follow-up.
Given the poor systemic status, conservative management to maintain the cerebrospinal fluid (CSF) pressure on the lower side with acetazolamide was advised. Over a course of 10 weeks, the swelling reduced but did not resolve completely (figure 1D). The patient unfortunately succumbed to her injuries.
Blepharocele is a collection of cerebrospinal fluid in the eyelid and may occur after head trauma. The first published case of CSF blepharocele was in 1957 by Bagolini.1 The postulated mechanism is a fracture of superior orbital rim along with a dural tear. The risk is greater children; in adults the well-developed frontal sinus may act as a buffer. Since the fluid is clear, the swelling trans-illuminates.
Conjunctival chemosis results from inflammatory oedema and is a common finding in the ophthalmic emergency room. A CSF blepharocele should be suspected if there is a non-resolving tense upper eyelid chemosis involving the palpebral conjunctiva more than the bulbar with an associated fracture of roof of the orbit. Imaging with cisternography can confirm the diagnosis. Aspiration with testing for Beta 2 transferrin levels though confirmatory for CSF, should be avoided as it may lead to brain herniation and/or meningitis.2 Most leak sites get sealed with inflammatory adhesions and blood products within 24–48 hours leading to spontaneous resolution.3 Repair of the causative dural tear may rarely be required for large tears. One should also look for associated CSF otorrhea and rhinorrhea.
Learning points
Cerebrospinal fluid leak into the upper eyelid is a rare cause of persistent chemosis after head trauma.
Tense upper eyelid swelling which trans illuminates should make the clinician suspect this rare cause of a common clinical finding.
Footnotes
Contributors SN: concept, data collection, manuscript preparation. AM: design, patient management, manuscript preparation. AL: patient management, data collection, manuscript editing and review. MD: concept and design, manuscript editing and supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.