Article Text

Statistics from Altmetric.com
Description
Tocilizumab is a new option in the treatment of giant cell arteritis.1 Based on normal acute phase reactants in the treatment of giant cell arteritis with tocilizumab, the detection of disease flare may be difficult.
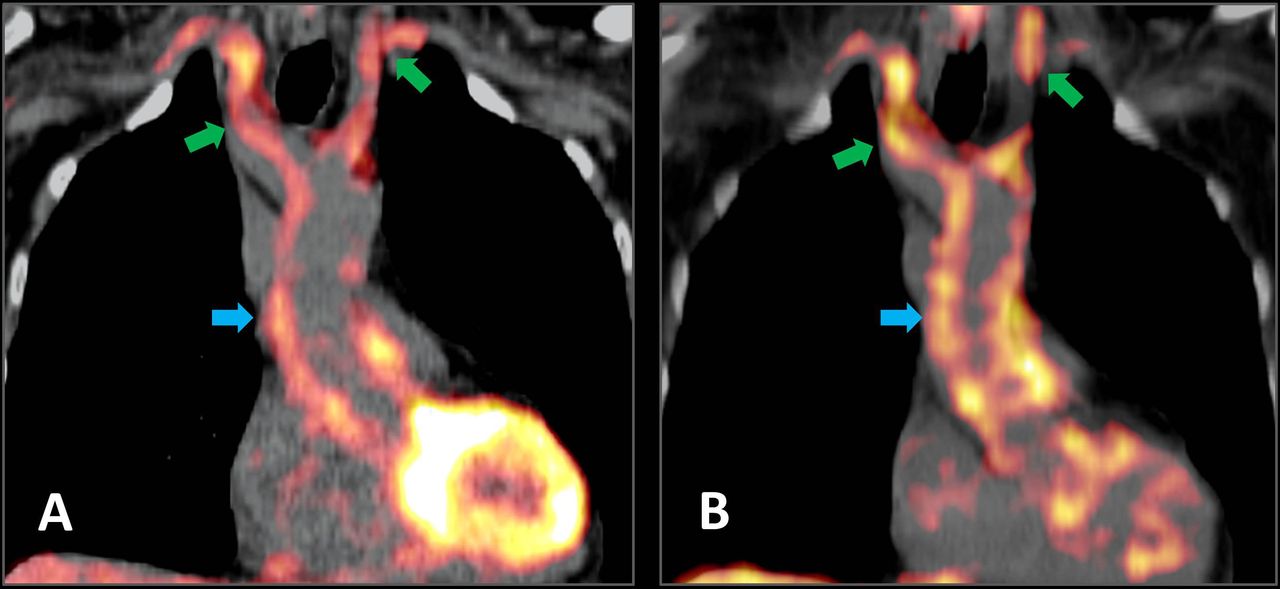
A 72-year-old woman was admitted to hospital with pain and stiffness of the shoulder girdle as well as occipital headache. The C-reactive protein (CRP) was 20.2 mg/L (reference: <2.0 mg/L). The power Doppler ultrasound showed a halo phenomenon of both common carotid arteries. The diagnosis based on the clinical, laboratory findings and ultrasound was giant cell arteritis. According to the clinical standard, a prednisolone therapy with 60 mg/day was initiated.2 All symptoms disappeared. After tapering prednisone to 40 mg per day, the patient presented a new onset of pain and stiffness in the shoulder girdle with occipital headache with a normal CRP. A (18)F-fluorodeoxyglucose positron emission tomography-CT (PET-CT) was performed for further evaluation and revealed inflammatory activity of the aorta, supraaortal arteries (see figure 1A) and the arteries of the upper and lower extremity. Consequently, the prednisone dose was increased to 60 mg/day and a therapy with tocilizumab was introduced. Prednisone was tapered in 26-week schema based on the GiACTA Trial.1 Two months later, the patient revealed anew pain and stiffness in the shoulder girdle associated with occipital headache. The CRP value was normal and the PET-CT showed again typical signs of giant cell arteritis (see figure 1B).
{kind=link}
(A) (18)F-fluorodeoxyglucose positron emission tomography-CT (PET-CT) presented inflammatory activity of the aortic wall (blue arrow) and supraaortal arteries (green arrows) indicating a giant cell arteritis resulting in the initiation of an tocilizumab therapy and (B) the (18)F-fluorodeoxyglucose uptake of the aorta and supraaortal arteries in PET-CT in association with anew pain, stiffness in the shoulder girdle and occipital headache under the therapy with tocilizumab revealed a flare of giant cell arteritis.
The case report describes a flare of giant cell arteritis, which was detectable by clinical symptoms and PET-CT imaging. In this context, CRP is no indicator for the detection of flare in the treatment with prednisone plus tocilizumab.3 The assessment of clinical symptoms in combination with imaging (eg, PET-CT) seems to be potential markers for the detection of a disease flare. Further studies were required to verify this finding.
Learning points
Clinical symptoms, in combination with imaging, are markers for the detection of giant cell arteritis flare.
CRP is not a marker for the dection of a disease flare.
Footnotes
Contributors AP, MFranz, GW and MFreesmeyer treated the patient, collected and interpreted the data and wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.