Article Text

Statistics from Altmetric.com
Description
A 63-year-old man with a history of hyperlipidemia and Gilbert's syndrome presented to the emergency department with subjective fevers, rigours and back pain, however normal vital signs. Laboratory evaluation was remarkable for elevated white cell count 19×109/L, C-reactive protein (CRP) 8.9 mg/dL and erythrocyte sedimentation rate (ESR) 110 mm/hour. Chest X-ray demonstrated bibasilar airspace disease. He received one dose of intravenous ceftriaxone and was sent home on oral azithromycin for presumed pneumonia. The blood cultures that were drawn at the initial visit grew group B streptococcus (GBS) in 2/2 sets within 24 hours. The patient was contacted to return for further evaluation. On day 3, he returned to the emergency department with worsening back pain. He was started on intravenous penicillin G and was admitted to the hospital. Searching for the source of his bacteremia, MRI of the T-spine was obtained; however, it only showed degenerative changes with disc osteophyte complexes (figure 1). Despite a negative MRI, suspicion for back infection was still high in the setting of severe back pain, elevated inflammatory markers and bacteremia. An 18-fluoro-2-deoxyglucose positron emission tomography (18F-FDG-PET)/CT was then performed and demonstrated hyper-metabolism of T7 and T8 vertebral bodies, suggesting infectious osteomyelitis (figure 2). The patient was diagnosed with T-spine osteomyelitis and his back pain improved with intravenous penicillin. Repeat blood cultures following penicillin infusion were negative. The patient was discharged home with penicillin G through a peripherally inserted central catheter line for 6 weeks in contrast to a much shorter course typically used for isolated GBS bacteremia. At the 3-week follow-up, his back pain completely resolved, ESR and CRP dropped to 49 and 0.28, respectively. Routine follow-up imaging studies were deemed unnecessary,1 given that he had improved symptoms with declining ESR/CRP.
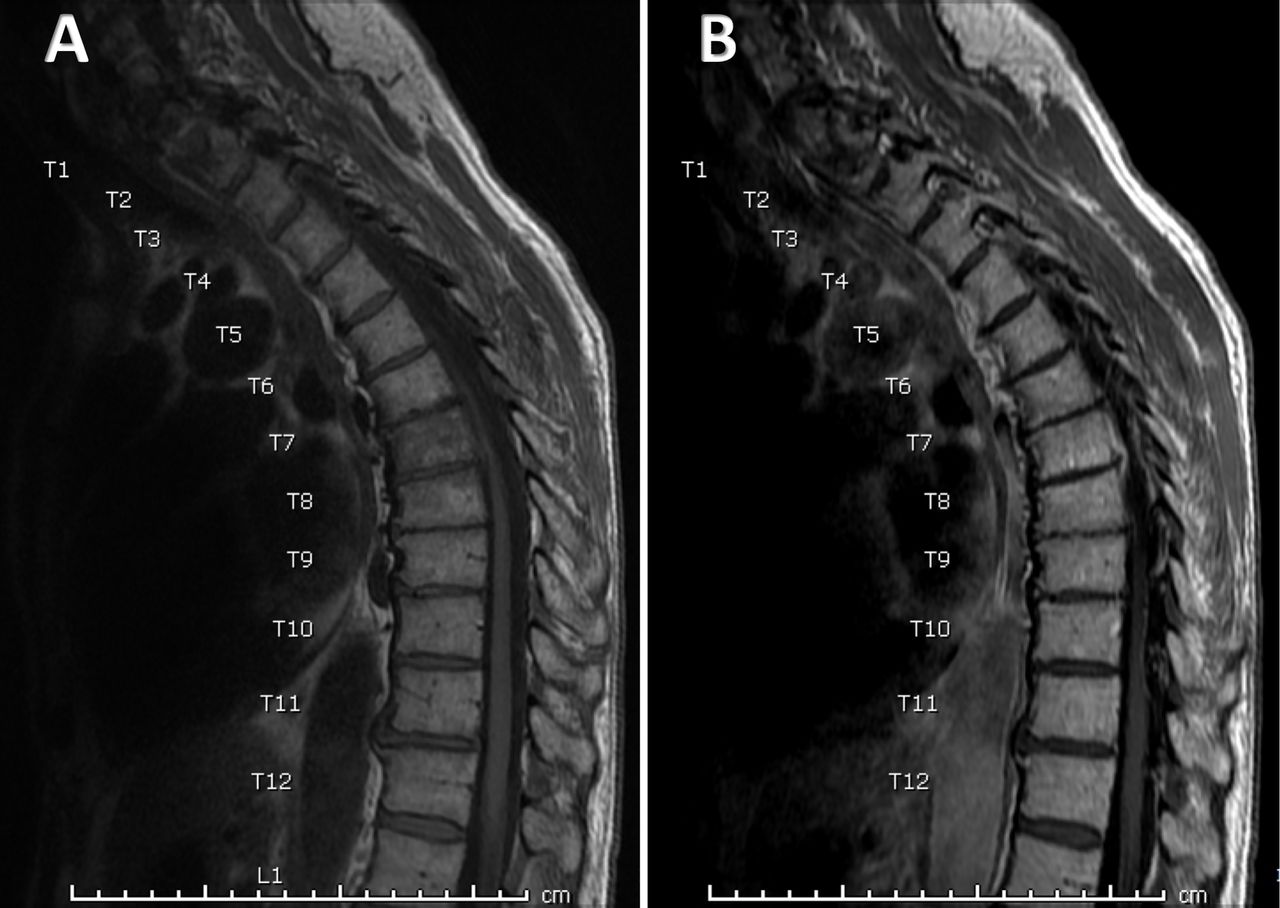
Sagittal T1-weighted MRI of the T-spine without gadolinium (A) and with gadolinium (B). No evidence of an epidural abscess was noticed. Enhancement of the T7 vertebra is secondary to disc osteophyte complex.
{kind=link}
{kind=link}
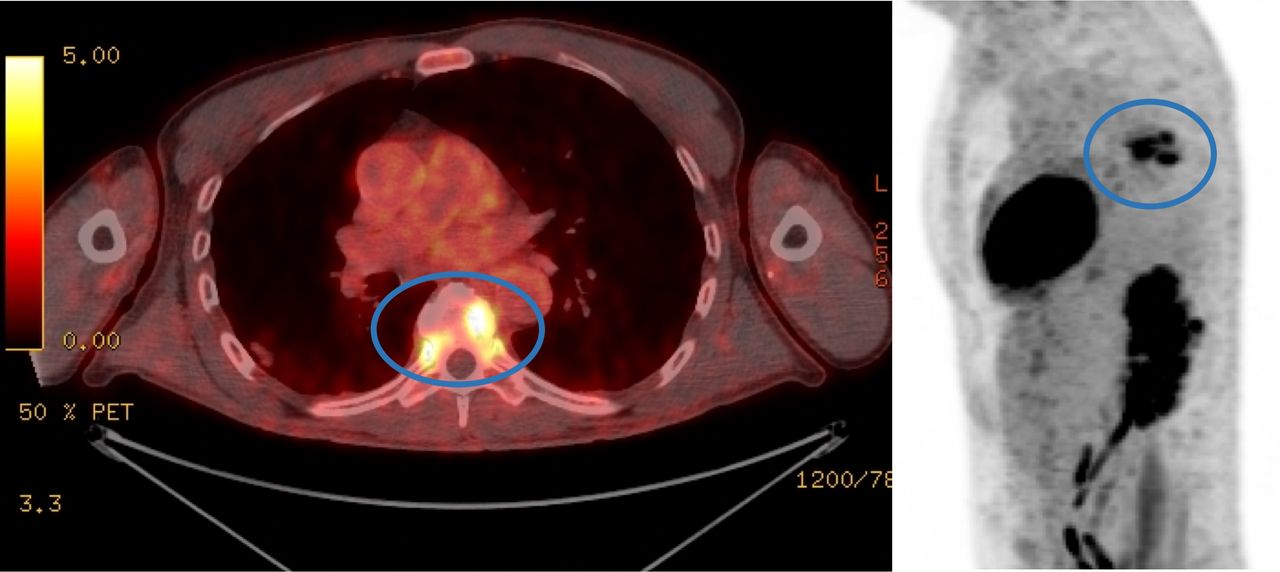
18-Fluoro-2-deoxyglucose positron emission tomography/CT: focal hyper-metabolism is noted within the T7 and T8 vertebral body endplates and within the intervertebral disc space demonstrating a maximum standardized uptake value of 6.5, concerning for osteomyelitis.
Vertebral osteomyelitis is a severe infection of the spine and may cause significant deformity and neurologic deterioration if left untreated.2 Early and accurate detection is essential for improving the outcome.3 MRI is the most often used radiographic technique for the diagnosis of vertebral osteomyelitis and is considered very sensitive.4 However, 18F-FDG-PET/CT has an advantage in the visualisation of metastatic infection,5 in patients with bacteremia, as shown in our case. Kouijzer et al4 reported 32 patients with suspected vertebral osteomyelitis who underwent both MRI and 18F-FDG-PET/CT, MRI was more useful for detection of epidural/spinal abscess, while 18F-FDG-PET/CT was more useful for detection of metastatic infection.
In general, biopsy is warranted to confirm clinical suspicion of vertebral osteomyelitis and to establish a microbiologic diagnosis. However, biopsy may not be necessary in patients with clinical and radiographic findings typical of vertebral osteomyelitis and positive blood cultures with a likely pathogen such as GBS.
In summary, this case emphasises that vertebral osteomyelitis can be missed in MRI of the spine, which is currently recognised as the standard diagnostic imaging for vertebral osteomyelitis. Considering the dire consequences of a delayed diagnosis, physicians should consider 18F-FDG-PET/CT to assist with the diagnose of vertebral osteomyelitis especially in patients with bacteremia.
Patient’s perspective
I strongly felt that my back pain was the underlying cause of my medical condition and was frustrated after my initial negative MRI. I was glad to know that the positron emission tomography (PET) scan was able to find the correct diagnosis, which allowed for proper treatment, and a peace of mind for me. I hope that this case can be published to alert doctors to the importance of considering PET scans in cases like mine that would otherwise be missed.
Learning points
MRI is the standard radiographic technique for the diagnosis of vertebral osteomyelitis. However, if the MRI is negative while clinical suspicion is still high, physicians should use 18-fluoro-2-deoxyglucose positron emission tomography (PET)/CT.
This case demonstrates the advantage of PET/CT for visualisation of metastatic infection.
Vertebral osteomyelitis should be highly suspected when a patient presents with fever, severe back pain with leucocytosis and elevated inflammatory makers.
Footnotes
Contributors ZLA has conducted significant research about the case, significant amount of planning and writing up the case and interpretation of the data; RB has discussed planning and reporting of the case with significant input in data acquisition as well as image interpretation; PB has contributed with data acquisition and reporting; JA has significantly contributed with planning, research, idea of the case and had significant contribution with data acquisition and image analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.