Article Text

Abstract
Upper gastrointestinal (GI) endoscopies are performed for several reasons. The overuse of endoscopy has negative effects on the quality of healthcare and pressurises endoscopy services. It also results in the complications. These complications include pneumoperitoneum, pneumomediastinum and subcutaneous pneumomediastinum. However, it is worth noting that these complications rarely occur during endoscopy of the upper GI tract. These complications, when they occur, indicate perforation of the retroperitoneal space or peritoneal cavity. In this article, we discuss a case of pneumoperitoneum, pneumomediastinum and subcutaneous emphysema after upper GI endoscopy.
- emergency medicine
- pneumomediastinum
- pneumothorax
- ultrasonography
- endoscopy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Excessive use of upper gastrointestinal (GI) endoscopy is increasingly becoming a global concern.1 According to estimates, about 56% of upper GI procedures are conducted inappropriately.2 3 Inappropriate use of upper GI endoscopy is accompanied by a risk of severe complications, high costs and low diagnostic yield.4 Dysphagia is difficulty swallowing, a common disorder, and an indication for several diagnostic procedures.5 6 Most cases of dysphagia are associated with oesophageal causes, thus requiring oesophageal-gastro-duodenoscopy (examination of the upper GI tract) as the primary examination. It has been established that inappropriate employment of upper GI endoscopy is associated with several risks and complications.6 Pneumoperitoneum, pneumomediastinum and subcutaneous emphysema are complications of upper GI endoscopy, which, however, occur in rare cases.7 This article presents a rare case of pneumoperitoneum, pneumomediastinum and subcutaneous emphysema after endoscopy of the GI tract.
Case presentation
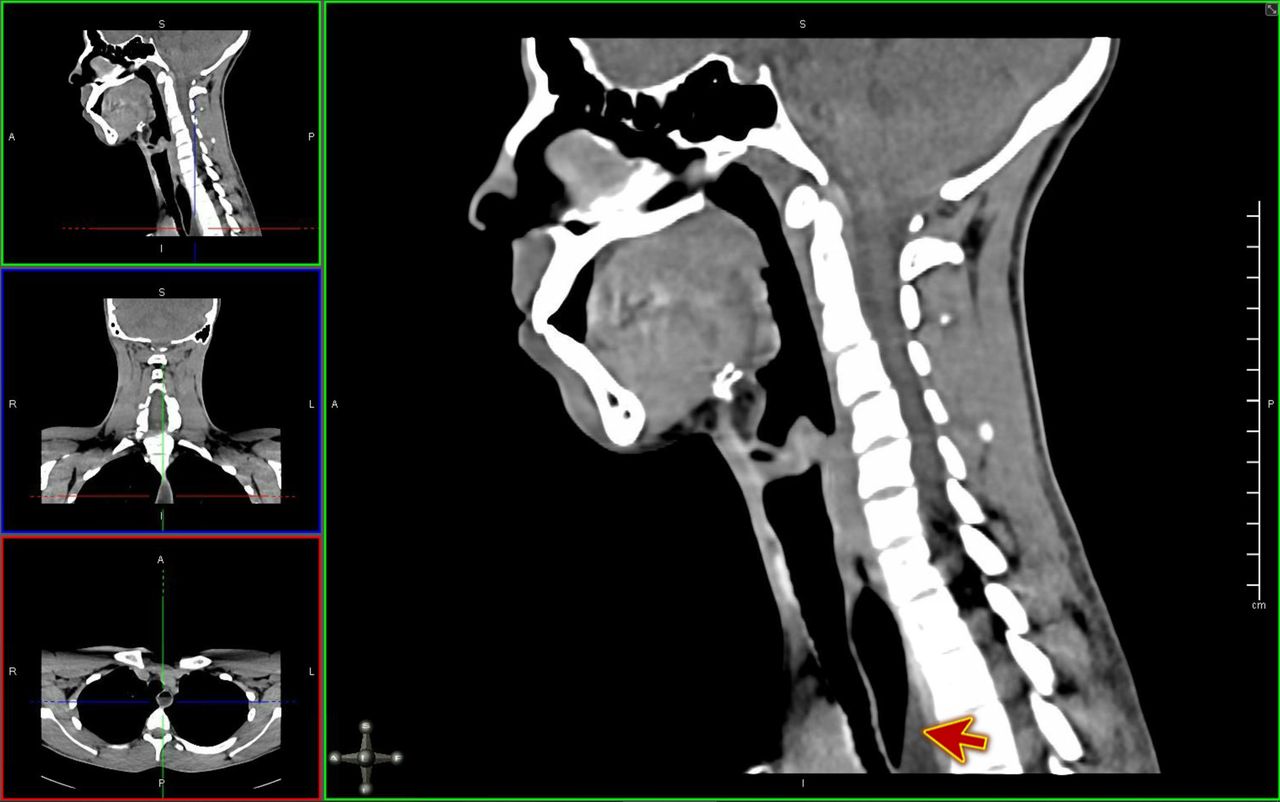
An 18-year-old male patient presented to the emergency department with dysphagia. The early morning before the presentation, he had eaten a piece of meat, after which he started to feel that something is stuck in his throat. He was extremely uncomfortable, and after many attempts, he spat part of it out. Since then, he was unable to eat or drink due to difficulty and painful swallowing. In the emergency department, he was vitally stable, and his physical examination was unremarkable. Fibre optic examination failed to detect any foreign body in the throat, so he was scheduled for CT of the neck, which showed an air-fluid level at the mid oesophageal part likely due to gastro-oesophageal junction abnormality (figure 1). He was assessed by the gastroenterologist in the emergency department and scheduled for upper GI endoscopy to rule out eosinophilic oesophagitis. The upper endoscopy showed a food bolus impacted at the distal end of the oesophagus and pushed down in the stomach with slight trauma to the mucosa (figure 2). During the procedure, the gastroenterologist noticed that that patient became tachycardic and developed surgical emphysema on the neck and cheek, so the procedure aborted, and the patient shifted back to the emergency department.

CT of the neck, which showed an air-fluid level (red arrow) at the mid oesophageal part likely due to gastro-oesophageal junction abnormality.

Upper gastrointestinal endoscopy showed abnormal mucosa of the oesophagus with furrows and narrowing with food bolus impacted at the distal end. The food bolus was pushed down in the stomach with slight trauma to the mucosa.
On arrival, his vital signs were as follows: the temperature was 36.6°C, heart rate of 123 beats per minute, with a blood pressure of 123/64 mm Hg, respiratory rate of 19 breath per minute and oxygen saturation 97% on room air. On physical examination, he was alert and oriented to time, place and person with a Glasgow Coma Scale of 15. There was an evident palpable surgical emphysema on the right cheek (figure 3), anterior neck and the upper anterior chest. The trachea was centralised, and chest auscultation revealed decreased air entry on the right-side chest compared with the left side. The rest of the physical examination was unremarkable.

Palpable surgical subcutaneous emphysema reaches on the right cheek.
Investigations
The white cell count was elevated to 17.3 ×109/L of blood with neutrophilic predominance. Other blood investigations, including electrolytes, blood gas analysis, kidney functions and liver functions, were unremarkable.
Differential diagnosis
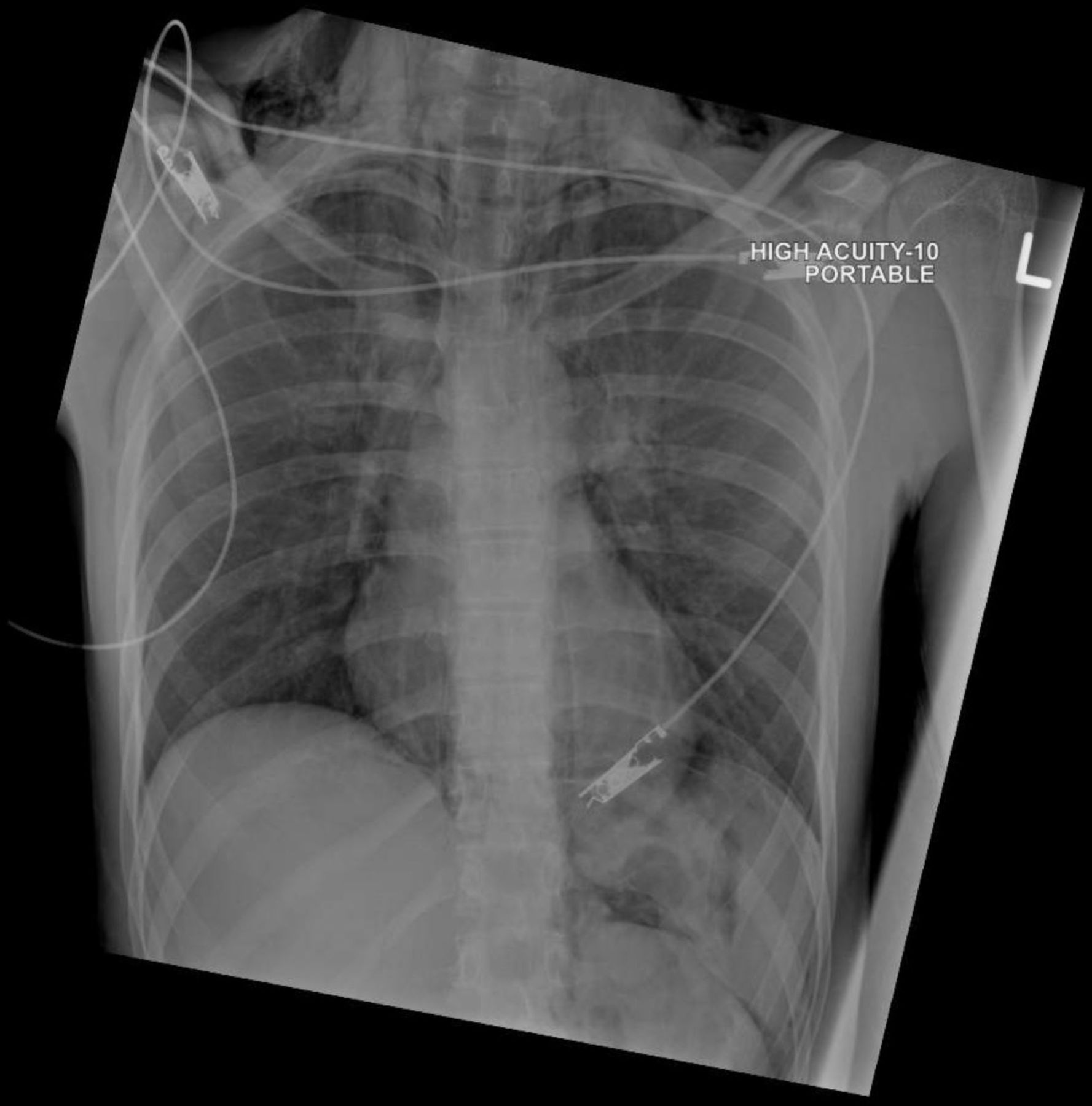
Chest point-of-care ultrasound (POCUS) was performed at the bedside and manifested the presence of right-side lung point (video 1), absence of pleural sliding, and M-mode barcode sign on the right side of the chest (figure 4). Chest radiography showed extensive subcutaneous emphysema, pneumomediastinum and small right-sided pneumothorax (figure 5). All these manifestations raised the concern for possible oesophageal perforation. So, the patient started on broad-spectrum antibiotics and sent for urgent contrast CT of neck and thorax with Omnipaque dye, which is water-soluble radiographic contrast. The CT revealed features suggestive of oesophageal perforation (interruption of the lateral wall of the lower oesophagus and faint contrast leak with the surrounding air at the site of the gastro-oesophageal junction). The CT also showed pneumomediastinum, right pneumothorax, pneumoperitoneum in the upper abdominal slices and subcutaneous emphysema, which extended to the right cheek (figures 6 and 7).

M-mode of the point-of-care ultrasound (POCUS) on the right side of the chest showing barcode sign (red arrow).

Chest X-ray showed extensive subcutaneous emphysema, pneumomediastinum and small right-sided pneumothorax. There is free air in the upper abdomen outlining the contour of the spleen and the left kidney.

Contrast CT of neck and thorax showing pneumomediastinum (blue arrow), right pneumothorax (red arrow) with surgical emphysema in the neck (green arrow) and pneumoperitoneum in upper abdominal slices (purple arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Contrast CT of the face and neck showing subcutaneous emphysema, which extended to the right cheek (red arrow).
Treatment
He was taken to the operation theatre by the GI surgeon for diagnostic laparoscopy, intraoperative upper GI endoscopy and laparoscopic feeding jejunostomy. The intraoperative finding was negative for gastric or oesophageal perforation with a negative bubbling test, but there was partial-thickness laceration at the distal oesophagus.
After the procedure, the patient was admitted to the surgical intensive care unit, and the pneumothorax was treated conservatively. A swallow test with oral contrast showed the free passage of contrast dawn to stomach without delay, contrast leak or extravasation.
Outcome and follow-up
After a few days, he stepped down to the surgical ward, and he started to tolerate oral fluid intake, the pneumothorax resolved without intervention, and he was discharged from the hospital with a jejunostomy feeding tube in place. The final histology from endoscopic biopsies confirmed the diagnosis of eosinophilic oesophagitis.
Discussion
Dysphagia is a Greek terminology that refers to ‘disordered eating’. Typically, the term dysphagia means difficulty in swallowing. It is an important and very serious symptom and requires a medical emergency when associated with chronic bleeding of the GI tract, dyspepsia, persistent vomiting, progressive unintentional weight loss, epigastric mass, deficiency anaemia and other upper GI symptoms. Several conditions affecting the upper GI may contribute to dysphagia. These conditions may be malignant or benign. Among these include structural or neuromuscular disorders that result in dysmotility of the oesophagus or oropharynx. Although the precise prevalence of dysphagia remains unknown, studies suggest that it may be within the range of 16%–22% after 50 years of age.7 8
The presentation of a pneumomediastinum is an indication that an air-retaining mediastinal structure has been breached. The air in the mediastinum tissues enters through the air passageway, for instance, after subjecting the pharynx to blunt trauma, hypopharynx, facial bones, main stem bronchi and the trachea. Dental care techniques, Valsalva manoeuvre, GI perforation and severe straining may trigger the appearance of subcutaneous emphysema and pneumomediastinum.8
In a freely perforated GI tract, air may flow into the mediastinum through the cavity of the peritoneum via the hiatus oesophagus, and also the Morgagni foramen. It is worth noting that pneumomediastinum in the absence of perforation has been observed after oesophagogastroscopy,9 colonoscopy or sigmoidoscopy,10–13 endoscopic sphincterotomy,8 14 endoscopic polypectomy and air contrast barium enema.15 16 Reports have also been issued describing pneumothorax for upper GI endoscopy.17–19
Probable explanations for the occurrence of subcutaneous emphysema, pneumomediastinum and pneumoperitoneum in our patient include injury to the afferent segment of the Billroth II gastroenterostomy or mucosa of the gastric mucosa by the endoscopic tip. This would allow entry of insufflated air into the wall. Pressurisation of the sensory segment of the Billroth II gastroenterostomy could contribute via allowance of forceful entry of air into the interstitium’s connective tissues.
A 1984 study by Maunder et al gave a graphical illustration of the channel that results in pneumothoraces and pneumomediastinum.20 There are four regions in the membranous compartment housing the neck, abdomen and the thorax—all defined as the visceral space, prevertebral tissue and subcutaneous tissue. The trachea is inverted by the oesophagus and the visceral space, continuing into the broncho-vascular and mediastinum sheaths. The trachea continues with the gullet (the informal name for oesophagus) through the diaphragm’s hiatus and penetrates the membranous space of the peritoneum and the retroperitoneum. Thus, there is a progression through the abdomen, neck and thorax. Airflow in these regions may arrive at another by flowing through the fascial planes.21
Kirschner offers another explanation. He suggested that peritoneal-pleural transphrenic movement of fluid and gases, either via acquired or congenital diaphragmatic pores, may be categorised as syndromes of the porous diaphragm.22
The patient, in our case, did not experience severe retrosternal discomfort. If any, it was mild. He had no difficulty in respiratory, considering that his respiratory rate was 19, although there was obvious, palpable surgical emphysema on the right cheek, anterior neck and upper anterior chest.
The most accurate tests for evaluation of subcutaneous emphysema, pneumoperitoneum and pneumomediastinum are those that enhance rapid determination of the size and location of perforation (if present), estimate the extent to which contamination has occurred, and assist the clinician in developing an effective plan of treatment. POCUS and plain X-rays of the abdomen and chest give a clear definition of the findings. However, issues bordering on relative insensitivity necessitates a CT scan of the chest, neck and abdomen. With a CT scan, the clinician can identify the origin of mediastinal air. Perforation may be detected with contrast-enhanced fluoroscopy of the oesophagogastric and pharynx regions. Evaluation of damage and management may be done with oesophagoscopy, bronchoscopy and laryngoscopy. Features suggestive of oesophageal perforation in our patient were revealed by urgent contrast CT of neck and thorax. It is worth noting that even with the examinations listed above, there may be a 5%–10% chance of the perforation remaining undetected, thus necessitating a repeat of the studies within a timeline of 12–24 hours. This will minimise the chances of an undetected perforation to below 2%.23
Patient’s perspective
While eating, I felt that the meat stuck somewhere in my chest. Doctors did for me an endoscope to remove it, but during the operation, I felt short of breath and surprised that my face was swollen. Doctors said to me that I developed air entrapment in my body, and they worked to solve that. I appreciate the efforts done by the doctors and nurses to save my life.
Learning points
Oesophageal perforation should be a suspected complication of upper gastrointestinal endoscopy and can lead to subcutaneous emphysema, pneumothorax, pneumomediastinum and pneumoperitoneum.
Point-of-care ultrasound is the first essential tool for detecting pneumothorax.
When undergoing evaluation for pneumomediastinum, conservative management should be applied. Oral administration is not appropriate at this time; instead, intravenous broad-spectrum and gastric aspiration antibiotics may serve the purpose.
Subcutaneous emphysema, pneumoperitoneum and pneumomediastinum following endoscopy may rightly be described as self-limiting, benign and without need for radiological or surgical intervention.
References
Footnotes
Twitter @amamiro2000
Contributors AE: clinical care, figures, manuscript writing, literature review. MH: manuscript review, literature review. KB: supervision. WAS: Manuscript review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.