Article Text

Statistics from Altmetric.com
Description
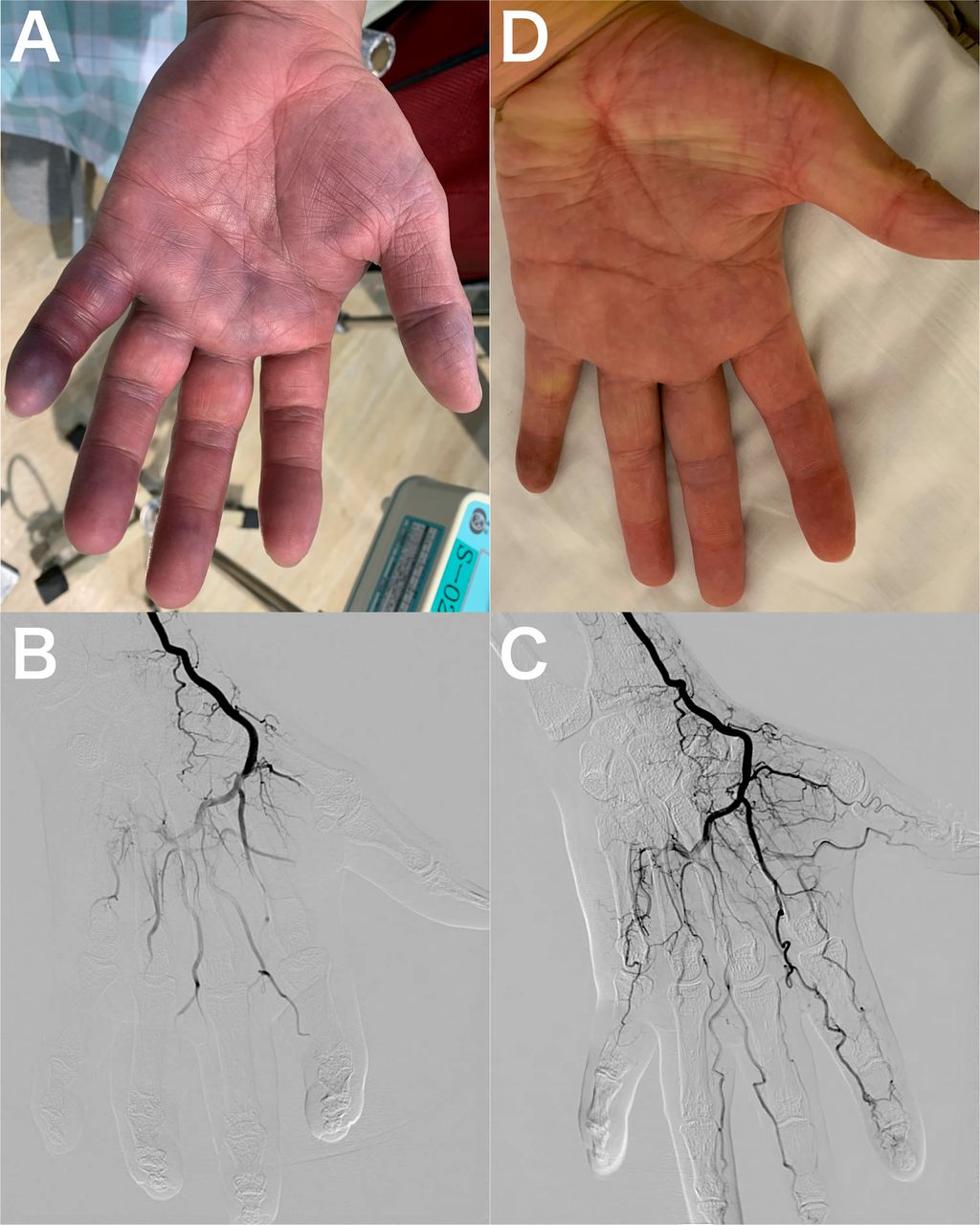
A 56-year-old man, an ex-smoker with thrombocytosis (undergoing treatment with aspirin) and hypertension, presented to the emergency department 18 hours after the sudden onset of left-hand cyanosis. He reported of an abnormal sensation and mild motor disturbance. His fifth finger showed severe cyanosis, while the other fingertips and palm showed moderate cyanosis without any ulcer and gangrene (figure 1A). Although his radial and ulnar arteries were palpated, his capillary refilling time was >2 s. We suspected acute upper limb ischaemia due to embolisation, considering his medical history. Therefore, we immediately administered a bolus of 5000 IU heparin followed by continuous heparin infusion and performed angiography via the radial artery, which revealed avascular fingertips, especially in the fifth finger (figure 1B). Since significant embolisation was not detected, we considered vasospasm. Therefore, we administered intra-arterial prostaglandin E1, which led to significant vasodilatation (figure 1C). Hand cyanosis markedly improved immediately (figure 1D). We prescribed an oral prostaglandin E1 derivative and a calcium channel blocker. Oral pain killer therapy and thermotherapy were also applied during the hospital admission. We considered regional nerve block as the next treatment strategy; however, its administration was deferred owing to the favourable clinical course of the patient. He showed no symptom recurrence for 6 months after the initial admission.
{kind=link}
(A) Hand findings before angiography, which indicates his fifth finger shows severe cyanosis, while the other fingertips and palm show moderate cyanosis. (B) An angiography via the radial artery before administration of intra-arterial prostaglandin E1, which reveals avascular fingertips, especially in the fifth finger. (C) An angiography after administration of intra-arterial prostaglandin E1, which leads to significant vasodilatation. (D) Hand findings after angiography, which show hand cyanosis immediately and dramatically improve.
Some reports suggested that accentuation of the sympathetic nerve system and cold stimulation caused the hand vasospasm.1 2 Therefore, performing an angiogram itself or arterial puncture could worsen the vasospasm. Although the patient required urgent attention, we should perform colour Doppler echography, which is a reliable modality for the transcutaneous assessment of blood flow in small vessels, for such patients. Emergent magnetic resonance angiography performed using optimised protocols is a considerably effective imaging modality for the non-invasive visualisation of the occluded arterial segments of the digital arteries without contrast,3 if available; however, this modality was not available in our institution. The use of these modalities before and after medical intervention could prevent the risk of contrast-induced vasospasm. Administration of sufficient local anaesthesia using a thinner needle and non-ionic–isosmotic contrast medium are also recommended to reduce the patients’ pain and subsequent accentuation of the sympathetic nerve system. To the best of our knowledge, we report the first case of hand vasospasm mimicking acute upper limb ischaemia. Hand vasospasm is a clinically important differential diagnosis for patients with hand cyanosis.
Learning points
Hand vasospasm is clinically important differential diagnosis of hand cyanosis.
The acute onset of hand cyanosis mimics acute upper limb ischaemia.
Angiography before and after intra-arterial prostaglandin E1 administration might be an effective examination and treatment with some attention.
Footnotes
Contributors KN wrote mainly this manuscript. KN and HA designed this concept. HA supervised it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.