Article Text

Abstract
A 77-year-old woman presented with right flank pain radiating to the ipsilateral groin and associated nausea, consistent with renal colic. In the emergency department, a non-contrast CT scan revealed severe right-sided hydronephrosis but failed to demonstrate a calculus or ureteropelvic obstruction. The patient improved with fluids and followed up with a community urologist. Initial work-up with cystoscopy and ureteroscopy, voiding cystourethrogram and diuretic renography failed to deduce a diagnosis. At our hospital, we used a modified dynamic (supine and upright) Whitaker test in a novel fashion to diagnose nephroptosis, a rare hypermobility condition of the kidney.
- urology
- urinary and genital tract disorders
- urological surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Nephroptosis is defined as descent of the kidney ≥5 cm or two or more vertebral bodies when the patient moves from a supine to an upright position.1 The condition is thought to be due to a deficiency in the support of the inferior renal fasciae and other perinephric structures. Hypermobility of the kidney has been documented in up to 20% of intravenous urograms of young adult women not experiencing symptoms; but a small, unknown proportion will experience symptoms from stretching or kinking of vessels, nerves or ureteral involvement during ptosis.2 A classic presentation (Dietl’s crisis) is characterised by acute abdominal pain and vomiting when the patient is upright that is rapidly alleviated when the patient moves to a recumbent or knee-chest position.2 The pain is localised to the flank with occasional radiation to groin, mimicking renal colic, and may be accompanied by nausea and emesis, intermittent haematuria and palpable flank mass.
Nephroptosis typically affects women (10:1 ratio compared with men) aged 20–40. Due to the rarity of the condition and asymptomatic predominance, the true prevalence remains unknown. Nephroptosis is a diagnosis of exclusion; supine and upright duplex ultrasound, intravenous urograms and radionuclide scans are commonly obtained if there is clinical suspicion. Diagnosis is suggested by sufficient renal descent between supine and upright positioning, development of obstruction when upright but not supine or imaging suggesting kinking of ureteropelvic junction or proximal ureter. Nephroptosis is typically treated with renal fixation via nephropexy.
The relationship between positive imaging studies and clinically significant disease is weak owing to the prevalence of asymptomatic nephroptosis; therefore, the use of a study that correlates ptosis and symptoms is critical. In this report, we examine the novel utility of a dynamic Whitaker test in the diagnosis of nephroptosis compared with previous diagnostic modalities. The Whitaker test is an anterograde urodynamic study used to determine the presence of mechanical obstruction, during which the renal pelvis is percutaneously accessed and infused with saline or contrast. Pressure monitors in the renal pelvis and the bladder are used to determine abnormalities.3 During the work-up of this case, we modified the Whitaker test to be performed both supine and in reverse Trendelenburg position to provoke and document positionally dependent obstruction.
Case presentation
A 77-year-old woman presented to her local emergency department with progressive right flank pain and associated severe nausea of 1.5 days duration. The pain radiated to the right groin and was worsened by movement. Initial vital signs were within normal limits and a comprehensive metabolic panel, complete blood count and urinalysis were unremarkable. An abdominal CT scan demonstrated severe right hydronephrosis of right kidney with perinephric stranding; no dilation of the ureter or urinary calculi was seen. She improved with intravenous hydration and antiemetics and was advised to follow-up with a urologist. One week later, she was seen by a community urologist who performed a technetium-99m mercaptoacetyltriglycine diuretic renography scan, which revealed delayed clearance and excretion of radionucleotide without clear evidence of obstruction (post-Lasix T1/2= 11 min). A voiding cystourethrogram was also obtained that revealed no vesicoureteral reflux or abnormalities of the lower urinary tract.
Five weeks following initial presentation, the community urologist performed a cystoscopy with right retrograde urogram and attempted ureteroscopy. A tortuous ureter was noted and the renal pelvis was not visualised; a double-J stent was placed and she was referred to our urologic service.
She presented to the University of Virginia urology clinic 7 weeks after initial presentation. With the stent in place, she reported nearly constant pain that limited her ability to complete daily 5-mile walks. The intensity of pain was exacerbated with movement, but it was not affected by hydration. One week later, she underwent right ureteroscopy with ureteral stent removal and placement of a right percutaneous nephrostomy tube that alleviated her pain. She was scheduled for a Whitaker test.
The patient returned in 2 weeks for a Whitaker test of the right renal pelvis and ureter, facilitated by the nephrostomy tube still in place. She was placed in supine position and dilute contrast was infused at a rate of 8 mL/min. Once 60 mL of contrast was infused into the renal pelvis, the patient reported mild flank discomfort and fullness. The differential pressure between renal pelvis and bladder was 15 cm of water, below the 20–22 cm of water cut-off for a diagnosis of obstruction.3 The patient was then placed in a reverse Trendelenburg position (45°) with continued perfusion of 8 mL/min. At this point, the differential pressure rose to 24 cm of water and she reported intense flank pain (figure 1). This dynamic study demonstrated positional-dependent obstruction via differential pressures and fluoroscopic imaging, supporting a diagnosis of symptomatic nephroptosis.
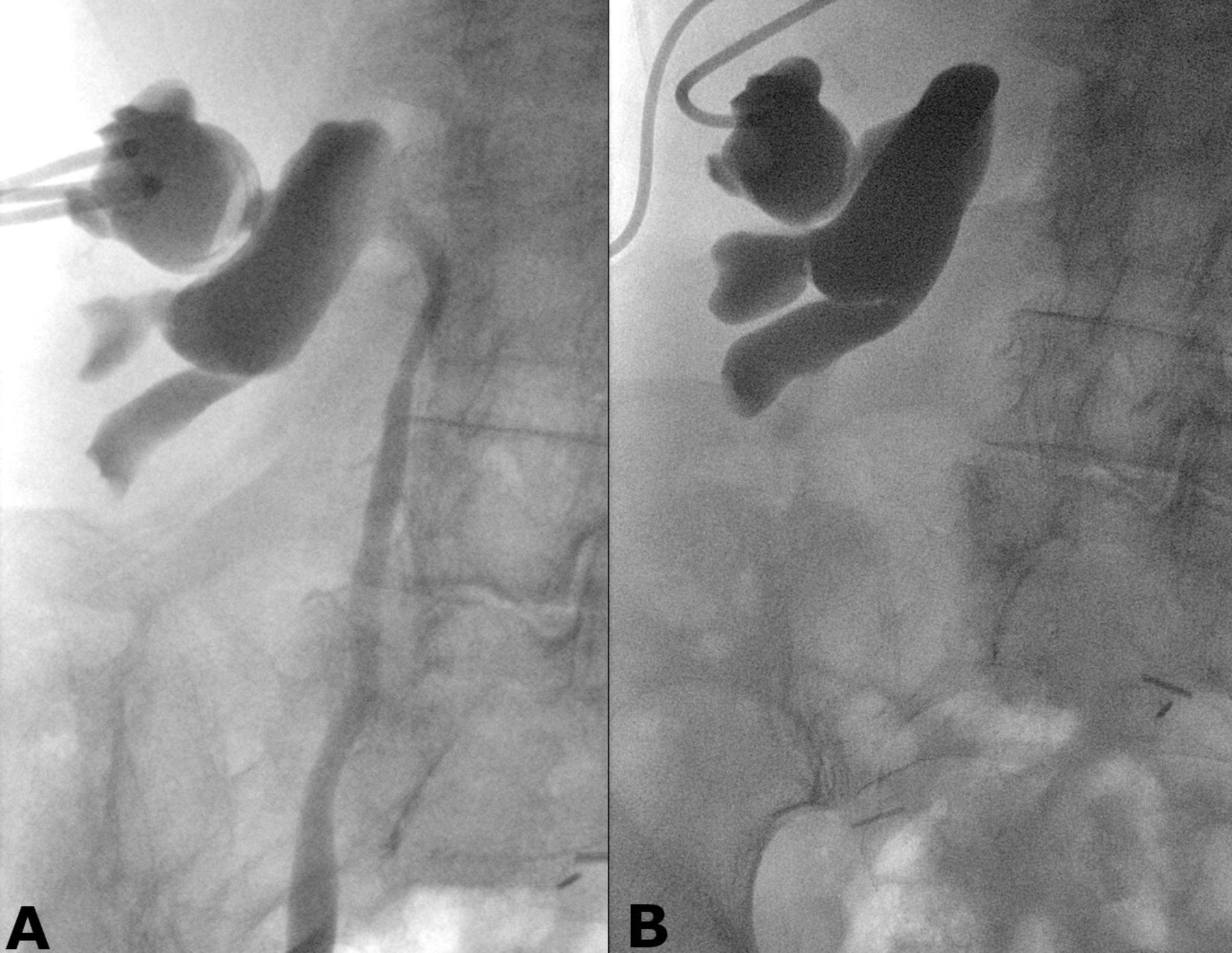
Coronal, anteroposterior fluoroscopic imaging obtained during dynamic Whitaker test. (A) Imaging obtained while the patient is supine; contrast is visualised in the pelvis and throughout the right ureter. No apparent narrowing of ureteropelvic junction or ureterovesicular junction. (B) Imaging obtained while the patient is in 45° of reverse Trendelenburg position; contrast is accumulating in renal pelvis without flow into the ureter.
The patient elected to undergo laparoscopic nephropexy, in which the right kidney is sutured and well approximated to the lateral abdominal wall. The nephrostomy tube was removed intraoperatively. Postoperative course was uneventful and the patient was discharged on postoperative day 1.
Outcome and follow-up
Two-month follow-up evaluation revealed a well-healed operative incision. She reported occasional lower back pain when walking longer distances, but flank pain had resolved. She denied any haematuria, dysuria or voiding complaints. One year following surgery, renal ultrasound showed complete resolution of right-sided hydronephrosis (figure 2).

{kind=link}
{kind=link}
Sagittal abdominal ultrasound of right kidney at 1-year post-op demonstrating complete resolution of hydronephrosis.
Discussion
Nephroptosis is a condition in which the kidney has increased mobility that may mimic renal colic in a position-dependent fashion.1 Dynamic imaging (supine and upright), which correlates symptoms to functional obstruction, remains the cornerstone in the diagnosis of nephroptosis. Our literature review revealed the common use of upright and supine ultrasonography, diuretic renography and intravenous urography in diagnosis; although its use has been posited, the Whitaker test has not been documented in the diagnosis of nephroptosis.4 Supine and upright intravenous urograms have historically been the standard diagnostic tool; however, diuretic renography and dynamic ultrasonography are complementary modalities that have been playing an increasing role in diagnosis. Diuretic renography is favoured as it can document renal obstruction via radiotracer excretion, decreased renal perfusion and/or changes in renal function.5 Nevertheless, diuretic renography has been found to be less sensitive than supine and upright ultrasound for diagnosing nephroptosis.6 Dynamic colour Doppler with estimation of renal artery resistive index (peak systolic velocity–end diastolic velocity/peak systolic velocity) has shown promise as a rapid and non-invasive test, with positive predictive power of 88%.6 In our ambiguous case with indeterminate diagnostic results from diuretic renography, we resort to a modified Whitaker test and propose it as a viable alternative to diagnose symptomatic nephroptosis.
The Whitaker test is a measurable analysis of the outflow resistance combined with radiographs that allows documentation of obstructive lesions and ptosis (which may help in preoperative planning).7 In contrast, the renogram examines renal function that may be due to obstruction combined with the information regarding the ease of radioactive isotope passage through the urinary system.7 In grossly dilated systems with poor renal function, the utility of renography is poor as it often incorrectly suggests obstruction due to isotope stasis; renograms also tend to miss obstruction in the presence of a solitary kidney with adequate function.7 In addition, the Whitaker test is a more provocative test as it is easier to induce positional obstruction by increasing the inflow during the test than by administering a heavier diuretic load during a renogram.7 Therefore, the higher predictive value for the Whitaker test in cases of intermittent or borderline obstruction vindicates its invasive nature. We propose that this modified Whitaker test can be a part of the urologist armamentarium in the diagnosis of symptomatic nephroptosis.
Patient’s perspective
I hope to never have such pain like that again. The paper you wrote is wonderful and I hope people learn from what happened to me to help people in the future.
Learning points
Nephroptosis is a rare condition that mimics renal colic in a position-dependent manner.
The standard tests for diagnosis include upright and supine ultrasound, intravenous urograms and diuretic renography.
A modified Whitaker test can serve to diagnose nephroptosis when traditional modalities are indeterminate.
Footnotes
Contributors RG collected all information regarding the case, performed the literature review, obtained the patient consent and composed the case report. NS directed care and served to inform the literature review and provide edits for the manuscript. MG performed the Whitaker test in this modified fashion; he also informed the literature review and provided edits to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.