Article Text

Statistics from Altmetric.com
Description
A 69-year-old man smoker with a prior medical history significant for severe haemophilia IX (B) on weekly factor-IX replacement and HIV, who presented with haemoptysis of a few hours duration.
Initially, the patient’s vitals were stable. Shortly after, he became altered with more haemoptysis and had to be intubated. Laboratory studies (table 1) showed low factor-IX levels, prolonged activated partial thromboplastin time and normal prothrombin time. A CT of the chest showed opacification of the right lung bronchi (figure 1). An emergent bedside bronchoscopy showed old clotted blood that was irrigated and suctioned, and a large endobronchial thrombus nearly occluding the right bronchus that was cleared until two small clots remained in the right upper and lower lobe segments. We decided to keep the remaining clots in place to ensure that the bleeding remained tamponaded. The patient’s saturation improved immediately with better compliance on the ventilator. Additionally, he was given factor-IX, factor-VII and intravenous as well as nebulised tranexamic acid. Moreover, he was started on intravenous vancomycin and cefepime due to the suspicion of aspiration pneumonia.

CT angiogram of the chest (coronal view), showing opacification of the right main stem bronchi with significant volume loss of the right lung. Infiltrates are noted on the right side. The endotracheal tube is also visualised (arrow).
Laboratory results at time of admission to the hospital
A second bronchoscopy was performed in the intensive care unit due to the continuous suctioning of blood through the endotracheal tube. It showed no active bleeding but an obstructing endobronchial lesion in the anterior segment of the right upper lobe that was biopsied (figure 2). Haemostasis was achieved using cold saline lavage. Pathology was negative for malignancy but revealed squamous metaplasia (SQM), acute inflammation and reactive changes associated with necrotic mucosa (figure 3). Repeat factor-IX levels were 202%, and no additional factor was given. Despite our efforts, the patient continued to have haemoptysis and failed multiple extubation attempts. We offered to transfer the patient to a specialised institution for bronchoscopic intervention; however, the family decided to proceed with comfort care measures, and the patient eventually passed away.
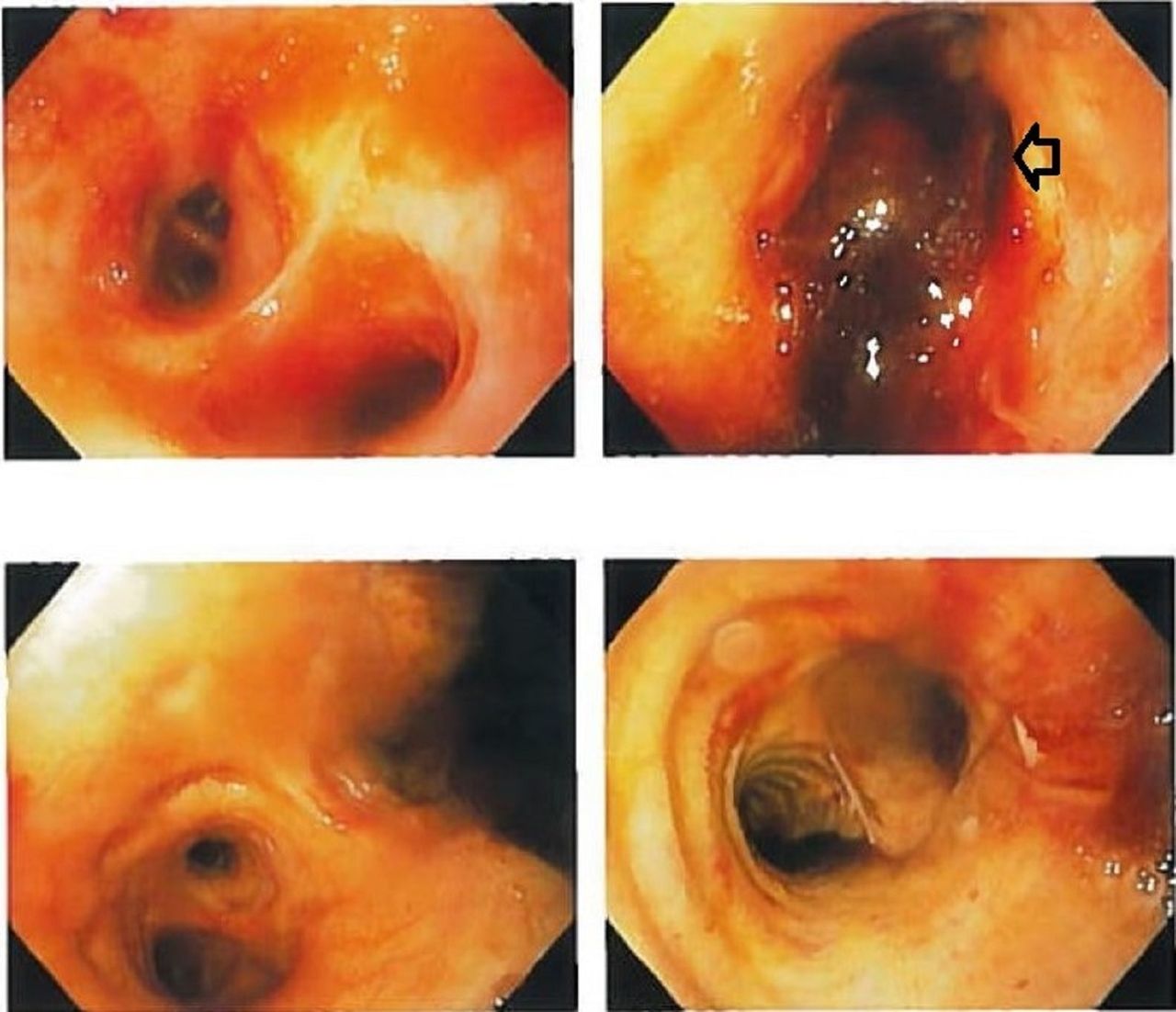
Bronchoscopy showing the right upper bronchus obstructive lesion that was biopsied (arrow head).

{kind=link}
{kind=link}
{kind=link}
Right upper lobe endobronchial lesion biopsy showing squamous metaplasia.
Haemophilia B is an X-linked factor-IX deficiency that can be divided into mild, moderate or severe depending on the plasma levels of factor IX: 5%–40%, 1%–5% and <1%, respectively.1 Spontaneous haemoptysis in patients with haemophilia is rare, and usually indicates the existence of an underlying condition such as neoplasia, pneumonia, endometriosis or chronic bronchial disease.2 Based on an article that reported five cases of patients with haemophilia presenting with haemoptysis, the author concluded that haemoptysis is usually limited to patients with haemophilia and end-stage HIV associated with severe bacterial or fungal infections.2 Our patient had a well-controlled HIV infection on medications with undetectable viral load and sufficient CD4 count. Moreover, he did not have any fungal or severe bacterial pneumonia, evidenced by negative respiratory cultures. However, he did have an endobronchial lesion with SQM that appeared to be the source of bleeding on bronchoscopy. SQM is a reversible preneoplastic transformation of the bronchial pseudostratified ciliated columnar epithelium as a result of an injury induced by smoking.3 Rigden et al reported an increase in SQM expression in smokers with chronic obstructive pulmonary disease (COPD) and suggested that this is a consequence of both smoking and COPD.3 SQM has been related to the intensity of smoking, defined as the number of cigarettes smoked per day; this result was not replicated by Rigden et al.4 Our patient did not have a formal diagnosis of COPD and never had a pulmonary function test. However, it is likely that our patient had undiagnosed COPD, given his prolonged history of heavy smoking. No association was found in the literature between SQM, haemophilia B and/or pulmonary haemorrhage. Symptomatic haemoptysis in haemophilia B should be managed by factor-IX replacement to achieve an initial level of 60–80 U/dL for 1–7 days and then a maintenance level around 30 U/dL for 8–14 days or until resolution of symptoms.5 Despite applying those measures, having sufficient factor-IX plasma levels and no factor inhibitors, our patient passed away, which proves that haemoptysis is challenging to manage in patients with haemophilia.
Learning points
Bronchoscopy should be done in any patient with haemophilia and hemoptysis as bleeding is unlikely due to the coagulation disorder itself, but due to another underlying lesion as in our case.
Haemoptysis typically occurs in patients with haemophilia and end-stage HIV infection and bacterial or fungal pneumonia.
Squamous metaplasia is a preneoplastic lesion that is caused by smoking-induced injury.
Footnotes
Contributors OM and FAR created the initial manuscript. CA and SK revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.