Article Text

Statistics from Altmetric.com
Description
A newborn boy, late preterm, with an uneventful pregnancy, presented with stridor and a systolic murmur since birth. A neonatal transthoracic echocardiogram revealed a patent ductus arteriosus and ostium secundum atrial septal defect. During the first year of life, he presented recurrent respiratory distress, cough, wheezing, stridor and multiple respiratory infections. For more than once, he required non-invasive respiratory support. Daily medication included inhaled steroids and montelukast but with poor response. He had an adequate development and physical growth, without feeding problems. A bronchoscopy was performed and a right distal tracheobronchial stenosis was identified.
At 18 months old, he was referenced to a tertiary paediatric cardiology centre, after the CT angiography showed an anomalous origin of the left pulmonary artery (LPA). The LPA originated from the proximal right pulmonary artery, coursing over the right mainstem bronchus, posterior to the distal trachea and anterior to the oesophagus, causing an airway compression (figures 1 and 2).

Transverse CT image after intravenous administration of iodinated contrast confirms the diagnosis of left pulmonary artery sling (LPAS; yellow arrow) arising from the right pulmonary artery (arrowhead).

A 3D-reconstructed CT image (posterior view) shows LPAS arising from the right pulmonary artery (RPA) crossing behind the trachea (Tr) causing stenosis. LPAS, left pulmonary artery sling.
He underwent surgical repair of the pulmonary artery sling (PAS) by median sternotomy. The LPA was repositioned to the left side of the main pulmonary artery, in the correct anatomical position, and the ductus arteriosus was ligated, under cardiopulmonary bypass, without tracheoplasty.
Postoperative bronchoscopy showed an improvement in the distal trachea caliber, without inspiratory collapse and incomplete cartilaginous rings. He was extubated on the first postoperative day showing a regression of the stridor, despite persistent respiratory distress. The patient was discharged 8 days after surgery and maintained a regular follow-up with an improvement of respiratory symptoms.
This rare form of vascular ring is known as PAS, which has an estimated prevalence of 59 per million school-aged children, but it is an underdiagnosed condition or misdiagnosed as respiratory pathology.1 Paediatricians must be aware of this cause of respiratory distress and have a high clinical suspicion index. It is associated with respiratory symptoms in the first year of life, due to tracheal stenosis, which can be life-threatening.1–3 Patients with tracheomalacia, recurrent or persistent stridor and/or wheezing should be evaluated for vascular rings, to allow an early diagnosis and timely surgical intervention, in order to avoid morbidity and mortality in children.
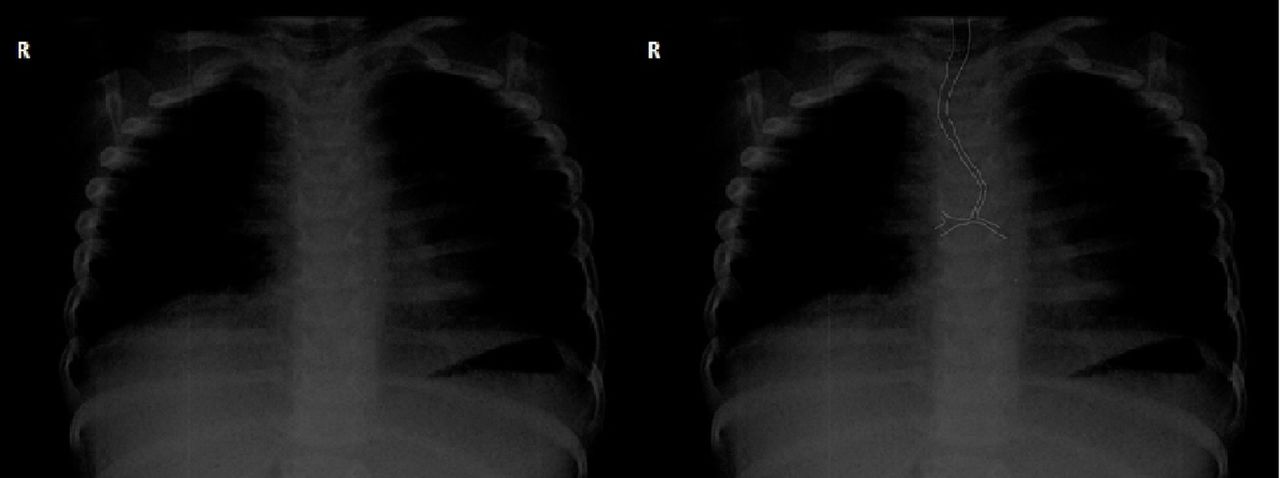
Retrospectively, the chest X-rays showed a narrowing and right indentation of the distal trachea (figure 3), which might have suggested the diagnosis.

{kind=link}
{kind=link}
{kind=link}
Chest X-rays show a narrowing and right indentation of the distal trachea.
Although echocardiography may be a helpful imaging tool, it is sometimes insufficient to establish this diagnosis due to its low sensitivity.2 CT angiography is the gold standard imaging technique providing not only an accurate diagnostic evaluation but also the best guidance for the surgical approach.3
Associated cardiovascular malformations are frequent, with a reported prevalence of up to 50%.3 This includes patent ductus arteriosus, which may contribute to encirclement of the trachea.
In symptomatic patients, the early reimplantation of the LPA to the anatomic position is effective. The clinical outcome is generally good, depending mostly on associated tracheal or/and cardiac anomalies.
Learning points
Patients with recurrent and/or prolonged stridor and wheeze should be examined for the possible presence of vascular rings and slings, such as pulmonary artery sling.
There must be a high degree of clinical suspicion regarding this diagnosis because it is a rare cause of respiratory distress.
CT angiography is the gold standard imaging technique. Early surgical management in symptomatic patients is effective.
Footnotes
Contributors NS: substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work and revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. TA: substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MCJ, DM: revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.