Article Text

Abstract
Takotsubo cardiomyopathy (TTC) is a rare but life-threatening condition that is still not completely understood. Characterised by rapidly reversible ventricular dysfunction without any prior coronary artery disease, it can imitate a myocardial infarction and lead to death if not managed appropriately. This report examines a case of intraoperative cardiac arrest in a patient with no previous cardiac disease, and discusses the factors that may have precipitated this event, as well as the ways of distinguishing the cause of the arrest based on clinical course and investigations, eventually leading to a diagnosis of TTC.
- cardiovascular medicine
- heart failure
- anaesthesia
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Takotsubo cardiomyopathy (TTC) is a rare but life-threatening condition characterised by transient left ventricular (LV) wall motion abnormality occurring in the abscence of coronary artery disease.1 First described in 1990, its presentation mimics an acute coronary syndrome (ACS) and is thought to comprise approximately 1%–2% of patients presenting with symptoms of ACS.2 While several mechanisms have been suggested to explain its pathogenesis, the most widely accepted hypothesis suggests a catecholamine surge causing a ‘stunning’ of the myocardium, leading to transient LV dysfunction.3 This is supported by stress (physical or emotional) being implicated as a trigger for TTC.4 The incidence of perioperative TTC is estimated to be 1/6700 cases.5 Diagnosis is typically based on meeting the clinical criteria as outlined by the Mayo clinic in 2008 (box 1).6 While other criteria have been proposed,7 the Mayo criteria is most widely accepted and used. Management is generally aimed at managing myocardial ischaemia with oxygen, anticoagulation (until a diagnosis of coronary artery disease is excluded) and beta-blockers.8
Mayo criteria for diagnosis of Takotsubo cardiomyopathy (reprinted with permission from Prasad et al6)
Transient hypokinesis, akinesis/dyskinesis of the left ventricular mid segments, with or without apical involvement.
Absence of obstructive coronary disease.
New ECG abnormalities -> ST elevation/T inversion or modest increase in troponin.
Absence of pheocromocytoma and myocarditis.
Cases of TTC are often associated with increased levels of serum catecholamines9 and therefore agents that increase catecholamines (such as Selective Noradrenaline Re-uptake Inhibitors (SNRIs)) may be a contributing factor in development of the condition. The report below outlines a case of perioperative TTC in a patient taking duloxetine along with other precipitating factors.
Case presentation
A 43-year-old woman presented for a surgical termination of pregnancy at 9 weeks’ gestation. She had a medical history of pneumococcal and streptococcal sepsis in 2009 with multiorgan failure, resulting in a below-knee amputation. She had tolerated previous general anaesthetics for multiple skin grafts and a splenectomy in 2009. She also had a significant autoimmune history, including autoimmune hepatitis, hypothyroidism, neuropathic pain and depression. There was no documented cardiovascular or respiratory history. Her medications included duloxetine 60 mg daily (which she had been taking for the past 5 years), thyroxine 100 µg daily and prednisolone 5 mg daily for her autoimmune hepatitis. While she had also been prescribed amoxicillin as part of the post-splenectomy protocol, she was poorly compliant with it. Her baseline investigations including thyroid function tests were unremarkable.
The procedure was planned under moderate to deep sedation. Standard monitoring was applied. Initial haemodyamic parameters included: heart rate (HR) 100 beats/min; blood pressure (BP) 90/60 mm Hg and oxygen saturation (SpO2) 97% on room air. Supplemental oxygen at 6 L/min was administered through a Hudson-type facemask with end-tidal carbon dioxide monitoring. Immediately prior to her procedure, she received intravenous 10 mg lignocaine, 600 µg atropine, 4 mg ondansetron and 75 µg fentanyl, followed by 50 mg of propofol to induce sedation. Once adequately sedated, the proceduralist injected 15 mL of 1% lignocaine and epinephrine 1:100 000 as part of cervical infiltration. The procedure was uneventful for the next 10 min, and she required a second dose of 50 mg propofol. Shortly thereafter, the SpO2 trace was consistent with a poor perfusion and a repeat (non-invasive) BP showed a reading of 55/30 mm Hg. Two boluses of 0.5 mg metaraminol intravenously were immediately administered but did not improve the BP, and her peripheral pulses were not palpable. Subsequently, four aliquots of epinephrine intravenously 25–50 µg were administered and additional peripheral intravenous access was established. With no change in her condition, cardiopulmonary resuscitation was commenced using standard Advanced Life Support (ALS) protocols. She achieved return of spontaneous circulation after 32 min of CPR. Interventions after return of spontaneous circulation included intermittent boluses of epinephrine to maintain BP, ventilation through a size 3 supra-glottic airway (SGA) (‘i-gel’) and establishment of a femoral arterial line. An epinephrine infusion was commenced at 0.2–0.3 µg/kg/min and a right internal jugular central line access was established. She remained in sinus rhythm with HR between 120 and 130 beats per minute. The first recorded invasive mean arterial pressure (MAP) was 60 mm Hg. Her MAP was maintained around 60–70 mm Hg with epinephrine and norepinephrine infusions 0.2–0.3 µg/kg/min. The post-resuscitation blood gas showed a metabolic acidosis with an elevated anion gap, consistent with a post-arrest state. Her hypokalaemia was corrected appropriately. The differentials considered at this stage were anaphylaxis, ACS or air/pulmonary embolism. Anaphylaxis was the primary differential at this stage, given the response to epinephrine; however, there were no other obvious systemic changes (ie, respiratory compromise, skin/mucosal tissue involvement) to indicate as such. A definitive airway was inserted to assist ventilation and facilitate ICU transfer. The procedure was allowed to continue, and on completion, she was transferred to the ICU.
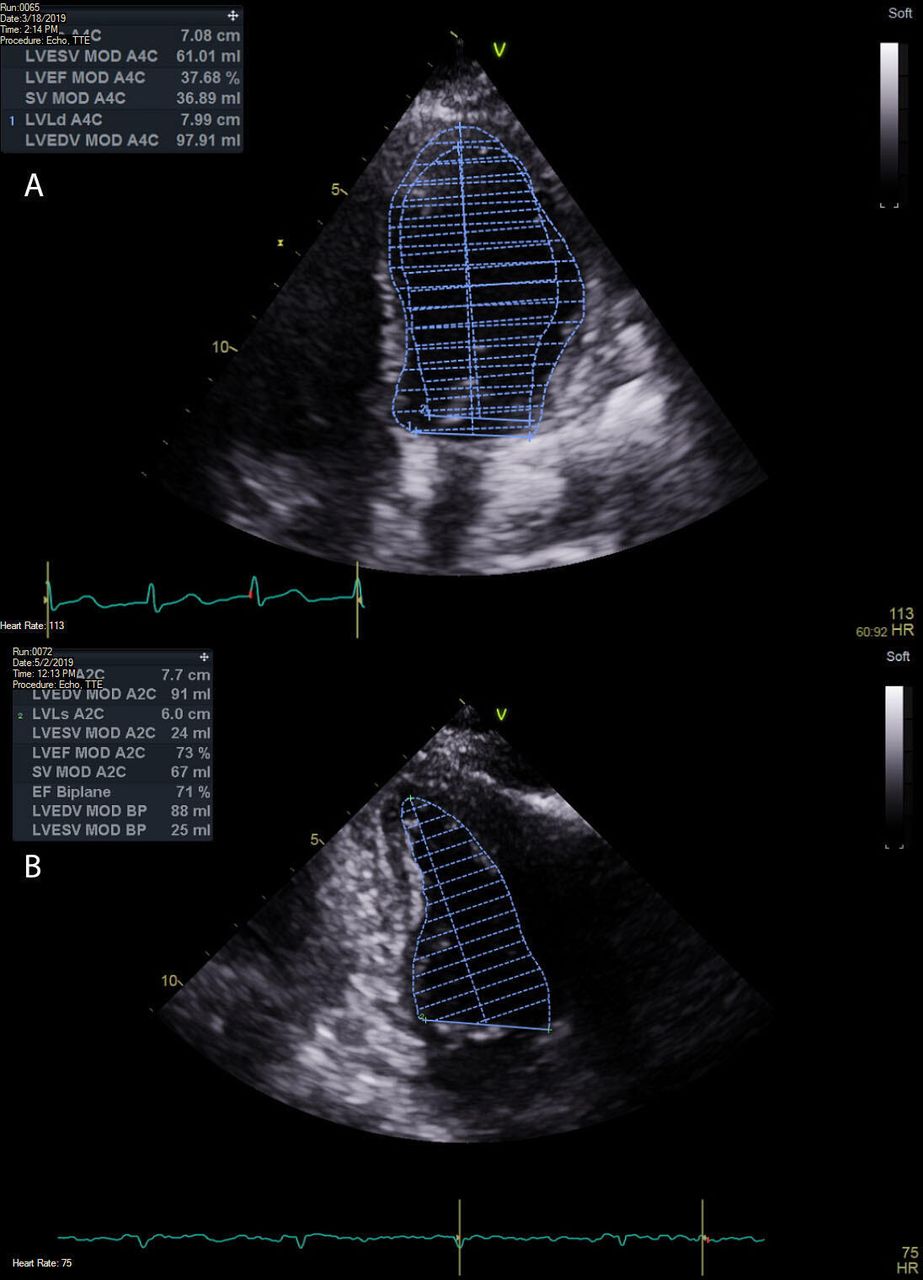
A 12-lead ECG in the ICU showed T-wave inversion in the anteroseptal leads and a corrected QT interval of ~500 milliseconds (figure 1). A bedside formal echocardiogram revealed a normal sized LV with reduced systolic function and an ejection fraction of 33% (figure 2). The Echocardiogram (ECHO) also demonstrated akinesis of the LV apex with mid-distal LV wall hypo/akinesis (video 1). She had normal right heart pressures, making a diagnosis of pulmonary embolism unlikely. Her echocardiogram findings were in keeping with acute cardiomyopathy. It was unclear at this stage whether this was secondary to intraoperative ACS/TTC or anaphylaxis and what specifically had provoked the event.
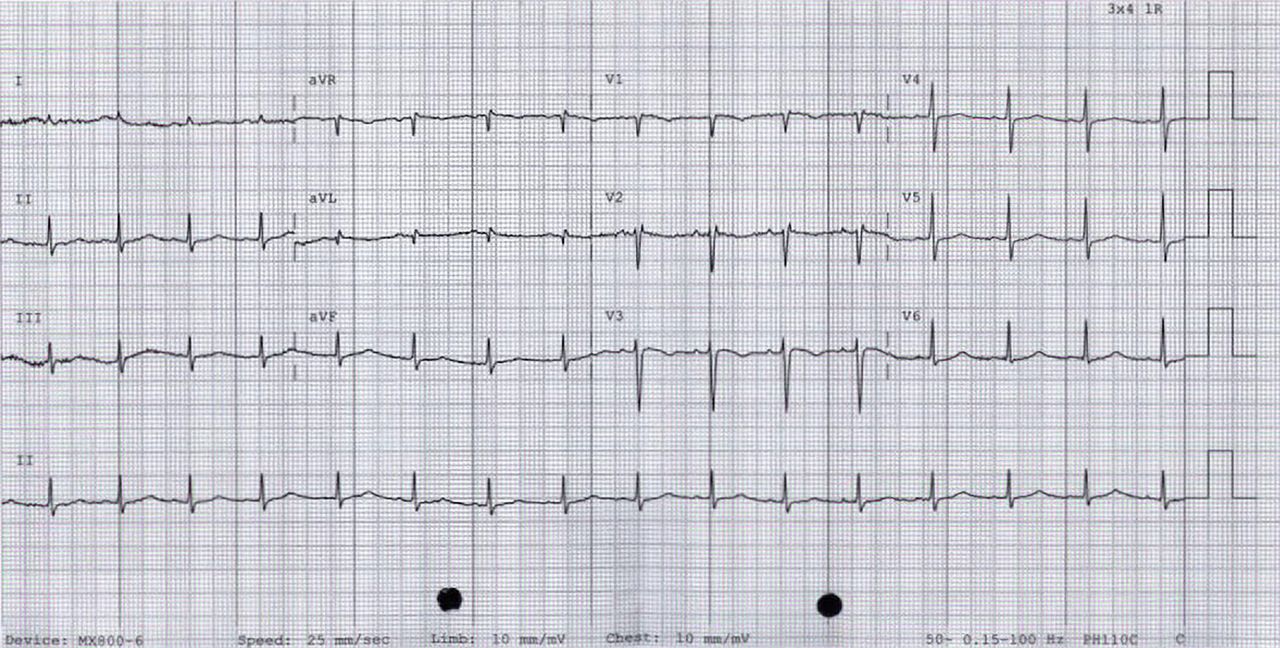
ECG immediately post event showing prolonged QTc (~500 ms) and T-wave inversion in leads V1, V2 and V3.

{kind=link}
{kind=link}
Echocardiogram results (A) immediately post event and (B) 3 months post event, showing an initial decrease in left ventricular function and subsequent improvement in function 3 months later.
Initial blood results showed normal tryptase levels of 4.8 µg/L (normal <11.9 µg/L) . Her tryptase levels continued to be normal at 4 hours post event (4.4 µg/L) and 24 hours post event (3.7 µg/L). Given the uneventful induction of anaesthesia, the patient was not exposed to any further potential antigens immediately prior to her acute deterioration to indicate anaphylaxis had taken place. Although these findings did not preclude a diagnosis of anaphylaxis, they made it less likely. The patient’s initial troponin T (TnT) was elevated to 0.191 µg/L, and 6-hour TnT was also elevated, however, began down-trending at 12 hours. While her initial N-terminal pro b-type natriuretic peptide (NT-proBNP) was normal at 98 ng/L, it was significantly elevated 16 and 40 hours later (table 1). Given the patient did not have any history of prior ACS or ischaemic heart disease, a preliminary diagnosis of TTC was given; however, this could only be affirmed with a repeat ECHO at 3 months showing a return of normal LV function (figure 2, video 2). It was thought that a combination of exogenous and endogenous factors (patient’s autoimmune history, medications, gender, operative stress, cervical infiltration of epinephrine) had all contributed to precipitate TTC.
TnT and NT-proBNP values taken on admission to ICU, 6 and 12 hours (TnT) and 16 and 40 hours (NT-Pro-BNP) post event
Outcome and follow-up
The patient was given an infusion of levosimenden in the ICU after consultation with the cardiology team, at 300 µg/hour, to optimise cardiac function and coronary blood flow. The catecholamines were weaned off over the next 12 hours. She remained stable overnight and was extubated the following day. She continued to make a full recovery and was discharged from the hospital 5 days later with a plan for outpatient cardiology review in 3 months time, with an echocardiogram to assess LV function prior to review. Repeat echocardiography at 3 months showed normal LV size and function, with an LVEF of 71% (video 2), helping to further affirm a diagnosis of TTC over ACS. Given the improvement in LV function and initial NT-proBNP changes, the cardiologist’s recommendation was that a formal angiography was not required at that stage to definitively exclude coronary pathology, and the patient would continue to receive ongoing cardiology follow-up and review as required.
Discussion
TTC is generally precipitated by exposure to endogenous or exogenous stress. Plasma catecholamine levels in patients with TTC are approximately two to three times higher compared with patients presenting with myocardial infarction, suggesting that this is the primary mechanism underlying TTC.9 It is hypothesised that elevated levels of catecholamines result in changes to intracellular signal trafficking, leading to negative inotropic effects seen maximally at the apex of the myocardium.3 Patients who present with TTC may have pre-existing endothelial dysfunction and reduced coronary artery reserve making them particularly susceptible to developing TTC during periods of acute stress,10 where circulating catecholamines are likely to be high. TTC tends to affect women predominantly; with about 90% of the cases of TTC involving women,4 however, it is unclear exactly why women are more susceptible to TTC.
The catecholamine surge results in LV dysfunction that is transient and reversible in nature.3 In the perioperative setting, there are a number of potential factors, which may contribute to the hyper-catecholeminergic state. Agarwal et al, in a review, identified factors such as inadequate depth of anaesthesia, exogenous administration of epinephrine, anaphylaxis secondary to release of inflammatory mediators (Kounis syndrome) and ergometrine use after caesarean as potentially contributing to a hyper-catecholeminergic state.11 Hessel estimated that TTC occurs in approximately 1/6700 cases.5 In Hessel’s review, of 131 cases, 37% presented during anaesthesia or surgery.
Perioperative TTC is more likely to present with evidence of heart failure, arrythmias or cardiac arrest5 compared with the classical TTC where the presentation is similar to an ACS. However, recognising TTC perioperatively and differentiating it from ACS can still pose quite a challenge. Use of cardiac biomarkers can assist diagnosis in this regard. Compared with ACS, TTC tends to have a much higher peak NT-proBNP and a lower TnT rise, and therefore, the peak NT-proBNP:TnT ratio has shown to be effective in differentiating between TTC and ACS.12 A ratio cut-off of 2889 for ST-elevation ACS and 5000 for non ST-elevation ACS has a 95% specificity for differentiating between those types of ACS and TTC.12 Our case shows this, with the patient’s peak NT-proBNP:TnT ratio being 12 919 (table 1), well above the aforementioned cut-offs for ACS. This ratio however is still only demonstrable post event and does not aid with recognition of TTC in the acute setting.
Duloxetine is a combined serotonin and norepinephrine reuptake inhibitor, and its effects are caused by increasing the levels of serotonin and norepinephrine at the neuronal synaptic terminals.13 Other SNRIs include venlafaxine and desvenlafaxine both of which are commonly prescribed for mood disorders. A systematic review of 22 cases of TTC by Hassan suggested that 14 of these may be induced by SNRIs.14 Patients with pharmacologically induced TTC tend to be younger compared with spontaneous TTC. They often also present without apical ballooning of the LV.14 There has been one reported case of TTC in the perioperative setting in a patient taking venlafaxine.15 We have not found a previously reported case of perioperative TTC in a patient taking duloxetine.
In our patient, the factors that may have contributed to an increased catecholaminergic state and subsequent TTC include: (1) long-term use of SNRI therapy; (2) emotional stress regarding the nature of the procedure and (3) exposure to exogenous catecholamines through injection of local anaesthetic mixed with epinephrine prior to starting the procedure. Other contributing factors include the patient’s gender and the history of autoimmune disease, which could precipitate endothelial dysfunction.
While the exact aetiology and pathophysiology of TTC may still defy explanation, a high index of suspicion should be maintained for individuals who have the above risk factors and have a subsequent intraoperative cardiac arrest. Supportive therapy is key to management of TTC, and tests such as NT-proBNP as well as serial echocardiography can be of significant benefit in helping to differentiate TTC from ACS.
Learning points
Takotsubo cardiomyopathy (TTC) can occur in the perioperative setting not only under general anaesthesia but under sedation as well. Other factors may include intraoperative epinephrine administration, inadequate depth of anaesthesia and pre-existing conditions contributing to TTC.
Use of NT-proBNP:troponin ratio can aid in differentiating TTC from acute coronary syndrome.
Supportive therapy is key in management of TTC.
A high index of suspicion for TTC must be present for patients who have a cardiac arrest with potential precipitating conditions, such as female gender, stress of event, pre-existing autoimmune conditions and patients who are on SNRI therapy.
Acknowledgments
The Queen Elizabeth Hospital, Department of Anaesthesia.
References
Footnotes
Contributors AJ: Manuscript preparation, formatting, data collection. JPR: Treating clinician, manuscript preparation, formatting, editing. VT: Treating clinician, report design, manuscript preparation, editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.