Article Text

Statistics from Altmetric.com
Description
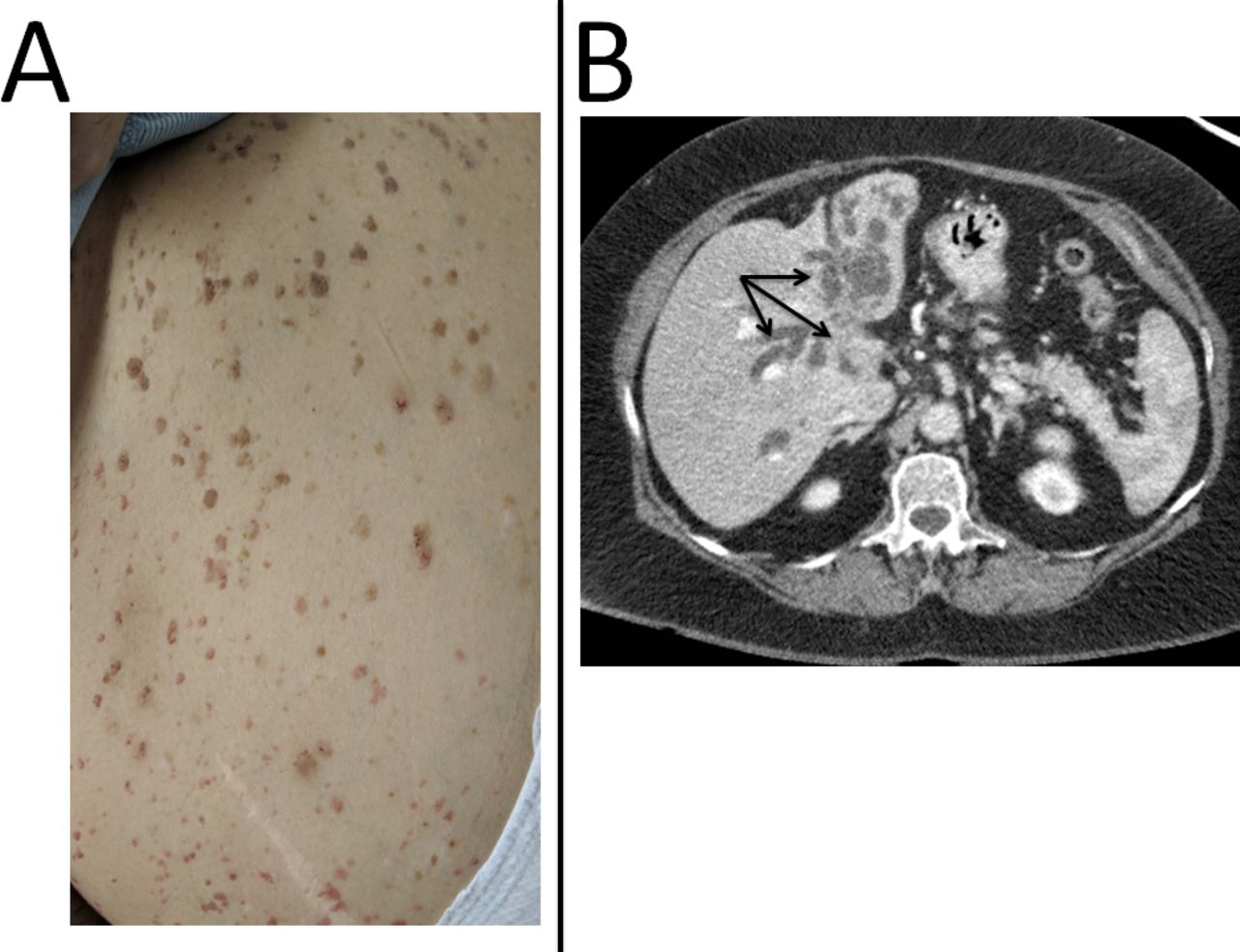
A female smoker in her seventies, presented to an emergency department with months of progressive weight loss, 1 week of worsening jaundice, pale stools and recent onset of episodic abdominal pain. Physical exam was notable for numerous seborrheic keratosis throughout the entire torso, ranging up to ~2 cm in size (figure 1 panel A). As seen in the accompanying figure the lesions ranged from a pale fleshy pink colour to darkly pigmented. The lesions occurred suddenly over the last 3 months erupting diffusely over her body. A triphasic CT was performed, identifying severe intrahepatic biliary ductal dilatation with an isodense poorly enhancing slightly heterogeneous ill-defined 2.7×2.2 cm mass at the confluence of the main intrahepatic ducts (figure 1 panel B arrows). The radiological diagnosis of Klatskin’s cholangiocarcinoma, was supported by an elevated CA 19–9 (48.7 U/mL).1 2 The obstruction was relieved with endoscopic retrograde cholangiopancreatography (ERCP); however, suitable tissue for pathological confirmation was not obtainable. This patient opted for palliative care, and sadly passed away months later.

{kind=link}
(A) Picture of patient’s abdomen on presentation demonstrating an example of the seborrheic keratosis of varying pigmentation consistent with the physical exam finding ‘The Sign of Leser-Trelat’. (B) A section of a triphasic CT using black arrows to highlight the isodense poorly enhancing slightly heterogeneous ill-defined mass consistent with cholangiocarcinoma.
This epithelial cell tumour typically have minimal and non-specific symptoms, therefore presenting with advanced disease.2 This patient’s initial eruptions of numerous seborrheic keratosis, is consistent with the rare exam finding ‘The Sign of Leser-Trelat’ (figure 1 panel A). This poorly understood exam finding, first described in the 1900s is an external manifestation of internal malignancy, most commonly gastrointestinal adenocarcinomas and rarely with cholangiocarcinoma.3–5 It is hypothesised that the eruptions are the results of cytokines and growth factors, such as epidermal growth factor alpha, produced by neoplastic cells.6 Despite controversy regarding the utility of the sign of Leser-Trelat given the prevalence of benign seborrheic keratosis with age, patient’s presenting with rapid widespread development of seborrheic keratosis, such as ours, should have occult malignancy on the differential. Notably with confirmed cases, the eruptions will often resolve with response to therapy of the underlying malignancy.
Learning points
The sign of Leser-Trelat is defined as the sudden eruption of of numerous, often multipigmented, seborrheic keratosis and should not be overlooked as a benign dermatological condition.
The sign of Leser-Trelat is a paraneoplastic syndrome often associated with adenocarcinoma of the gastrointestinal tract and lung, and less commonly with hematological malignancies.
While cholangiocarcinoma often presents late in its disease course, due to vague symptoms, in a rare subset of cases it manifests with paraneoplastic symptoms.
Footnotes
Contributors AM and AA contributed equally to the preparation of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.