Article Text

Abstract
Acute traumatic intra-articular dislocation of the patella is not a common presentation in orthopaedic practice; less frequently observed than extra-articular dislocation of the patella. In some of these cases, closed reduction is not possible and an open reduction in the operating theatre must be performed. In this case report, we present an elderly patient with an intra-articular horizontal dislocation of the patella without any other bony or ligamentous lesions seen in a postreduction MRI. We conducted a literature review looking at intra-articular patella dislocations, identifying 64 published studies (articles, case reports and papers). The following sources of data were searched until December 2017: PubMed, OVID, Google Scholar, Scopus, using the search strategy of (intra-articular dislocation of patella, horizontal patellar dislocation) with no limitation on the year or language of publication. The patient presented in this case report was managed with a closed reduction under general anaesthesia, without the need of any surgical intervention. As proposed in the literature, the hypothesis of an intra-articular entrapment of the patella due to the trapped osteophytes of the superior pole of the patella into the intercondylar notch was thought to be the cause of intra-articular dislocation in this elderly patient.
- orthopaedics
- patellofemoral pain
- orthopaedic and trauma surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
This case report serves to highlight this infrequent trauma presentation in the elderly population as well and to remind medical practitioners that although rare, dislocation of the patella should be suspected in the case of locked knees, especially in patients with known osteoarthritic changes.
Case presentation
A 92-year-old woman presented to the emergency department of Insel hospital in Bern, after a direct trauma to her right knee postmechanical fall. The patient presented with a locked knee in 100° flexion and was unable to actively extend her knee. X-rays revealed an intra-articular dislocation of the patella with an entrapment of the upper pole in the intercondylar notch (figures 1 and 2). A fracture was not visible on the plain radiograph. The patient had a successful closed reduction of her intra-articular patella dislocation under a general anaesthetic. The closed reduction was straightforward, with direct pressure placed on the inferior pole of the patella and the knee put in flexion. The manipulation under anaesthesia was performed in the operating theatre as it was uncertain if a closed reduction would be possible. A cylindrical cast was applied for 3 days postprocedure, until the postreduction MRI was done to exclude any traumatic pathologies. The clinical examination after reduction revealed no haemarthrosis, no palpable dehiscence in the quadriceps tendon and an intact straight leg raise test.

Lateral X-Ray of the affected knee.

Sunrise X-Ray of the affected knee.
Investigations
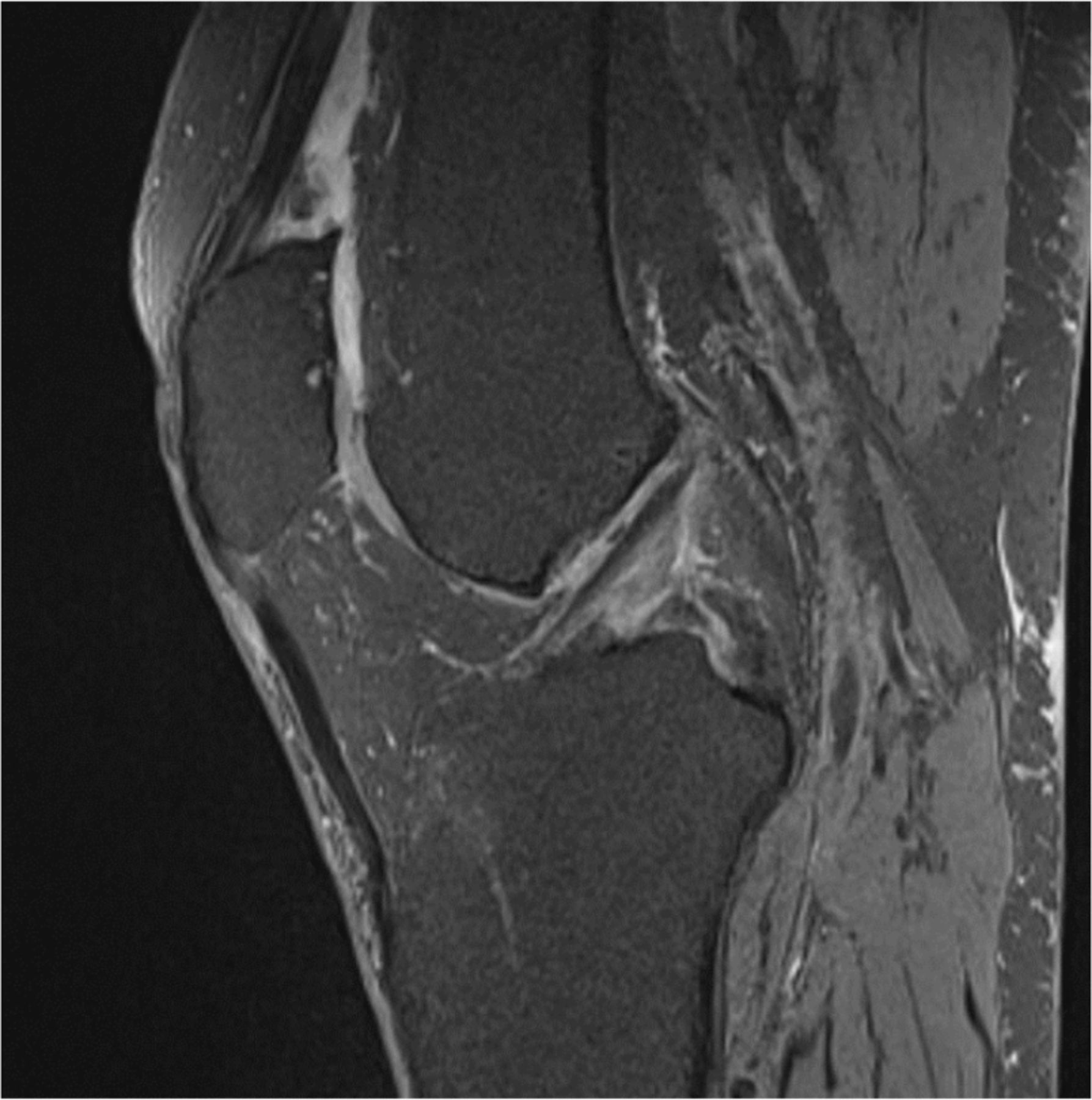
The postreduction X-rays (figure 3) showed adequate positioning of the patella in the trochlear groove. The patellar height was measured at 1.2, using the Caton-Deschamps index.1 An MRI (figure 4) postreduction was performed and revealed no intra-articular pathology, with an intact quadriceps tendon and no intra-articular fragments. The MRI did however identify the presence of osteophytes at the superior pole of the patella and in the intercondylar notch, confirming the hypothesis of an intra-articular entrapment of the patella due to the trapped osteophytes of the superior pole of the patella into the intercondylar notch.

Post-reduction X-ray.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI of the knee after reduction which shows an intact quadriceps tendon and the presence of the presence of osteophytes at the superior pole of the patella.
Differential diagnosis
As the osteophytes appeared to be the reason for the dislocation, we considered an arthroscopic resection for further management of this patient, to help prevent further dislocations. The poor prognostic factors for further surgery were the patient’s age and normal mobility status.
Treatment
Physical therapy was initiated on day 1 postprocedure, with weight bearing as tolerated in crutches and on the day of discharge, the patient was able to walk normally without the aid of crutches or need for a brace. After a 3-day admission, the patient was discharged from hospital.
Outcome and follow-up
In last outpatient follow-up, 1-year postinjury, she presented with full preinjury function of her knee, with no further recurrence of the dislocation and could return to her activities of daily living approximately after 6 weeks.
Discussion
This rare condition was first described in the literature by Midelfart.2 Since 1887, 64 cases of an intra-articular patella dislocation have been reported in the world literature.3–60 Intra-articular dislocations of the patella are separated in two groups: horizontal and vertical, according to the axis of rotation. The horizontal dislocation is more common and occurs after a direct trauma on a partially flexed knee, which leads to a rotation of the patella around its horizontal axis. When the knee joint is in flexion, the upper pole of the patella lies in front of the intercondylar groove, the initial traumatic blow, if exerted on the upper pole, pushes the patella posteriorly and it may lock in flexion.3
Horizontal rotation can detach the quadriceps tendon from the upper patella pole, and the articular surface faces distally to the tibia plateau. Less frequently, the lower pole of the patella tears away from the patellar tendon and becomes locked within the joint, with its articular surface pointing proximally.37 38 56 57 In the less common vertical type of dislocation, the patella rotates on its vertical axis, with the edge lying in the notch. The articular surface faces medially or laterally, and the patient presents with the knee in near full extension.61 62
According to our bibliographical analyses, the majority of the dislocations (58%, 37/64 patients) underwent an open reduction,21–54 whereas only 31% (20/64 patients) could be reduced with a closed reduction.3–11 55–61 In the other 11% of cases, the reduction and anaesthesia methods were not clearly mentioned. Murakami35 has proposed that successful manipulative reduction depends on the degree of locking of the patella within the joint. Although successful closed reductions have been reported under sedation with ethonox,4 chloroform36 and even with intra-articular anaesthetic solution,55 the importance of general anaesthesia with adequate muscle relaxation has been emphasised to prevent any further chondral damages.6
The mean age of the patients with this rare pathology was 31.9 years (range 9–93 years). The mean age of patients who underwent an open reduction was 22.4 years (range 9–88 years) and the mean age of patients with closed reduction was 45.3 years (range 10–93 years). It is becoming clear that a successful closed reduction under anaesthesia may be expected in the elderly group, in whom the dislocation is liable to occur owing to osteophyte locking rather that true impaction of the patella and the injury mechanism does not involve a high energy trauma.
An open reduction allows an inspection of the soft tissues and accurate repair if needed and should remain the preferred treatment for intercondylar patellar dislocation in young patients where the mechanism force is more important and an associated soft tissue injury more likely to happen due to lax patellar attachments.22
Learning points
Our case demonstrated that the patella had dislocated horizontally, and the reason of the entrapment was considered to be the osteophytes of the superior pole of the patella in the intercondylar groove.
This case report serves to highlight the existence of this rare condition in the elderly population as well and to remind medical practitioners that although rare, dislocation of the patella should be suspected in the case of locked knees, especially in patients with known osteoarthritic changes.
An open reduction allows an inspection of the soft tissues and accurate repair if needed and should remain the treatment of choice be intercondylar patellar dislocation in young patients where the mechanism force is more important and an associated soft tissue injury is more likely to happen.
Previous case reports confirm that the extensor mechanism usually remains intact as in our case but there can be varying degrees of quadriceps tendon avulsion.5 29 Six (6/64) patients with intra-articular dislocation were found to have an associated avulsion of the distal quadriceps tendon,8 22 27 29 42 51 one of them had additionally a medial patellofemoral ligament tear,22 whereas one case had a coronal shear femoral Salter-Harris type III fracture in a 15-year-old boy.59
References
Footnotes
VD and LG are joint first authors.
VD and LG contributed equally.
Contributors LG and VD searched, analysed the literature and wrote the case report, have the full responsibility of the design and the acquisition of the data, VD also obtained the consent form, ZJ has revised the case report, JW has revised, verified the quality of the case report and finally approved the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.