Article Text

Statistics from Altmetric.com
Description
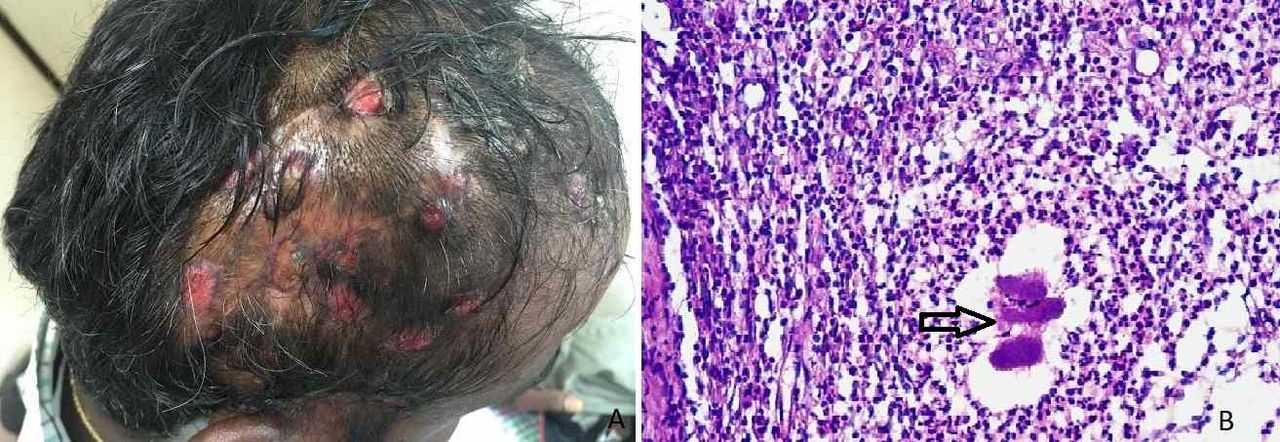
A 36-year-old man who had previously sustained multiple bruises on his scalp due to a road traffic accident that had healed spontaneously, reported with multiple, painless, greenish pus draining sinuses at the same site since 8 months. There were no systemic symptoms. Local examination confirmed the same with sinuses having pouting granulation tissue and no bony tenderness or fractures (figure 1A). Occipital non-tender lymphadenopathy was present.

{kind=link}
(A) Multiple sinuses of the scalp; (B) Photomicrograph showing actinomyces (black arrow), H&E ×40.
Tuberculous osteomyelitis was suspected and pus sent for Gram stain, culture and GeneXpert, but was not contributory. Mantoux test was also negative. Skull radiograph showed a thickened parietal vault and intact inner table, but multiple defects in the outer table suggestive of chronic osteomyelitis. A punch biopsy from the granulation tissue done showed foci of sulfur granules comprising of filamentous basophilic radiating fungal-like structures in the dermis surrounded by acute and chronic inflammatory cells, namely, neutrophils, plasma cells and foamy macrophages intervened with fibroblasts representing actinomyces (figure 1B). Fine needle aspiration cytology of the occipital lymph nodes was inconclusive.
Actinomycosis is a rare, chronic bacterial anaerobic infectious disease caused by Actinomyces species (ray fungus), which is ubiquitous and occurs in soil and in the microbiota of animals and humans.1 It is characterised by contiguous spread, suppurative and granulomatous inflammation, and formation of multiple abscesses and sinus tracts that may discharge sulfur granules.2 Common clinical forms are cervicofacial, thoracic and abdominal and in women, pelvic actinomycosis.3 Tuberculous osteomyelitis mimics actinomycosis, causing a diagnostic dilemma and only a biopsy can confirm the diagnosis. The patient was started on penicillin G and sinus tracts were excised. At a follow-up visit, 1 month later, the sinuses have healed well but with fibrosis and patchy alopecia.
Learning points
Actinomycosis is a granulomatous bacterial infection.
It can mimic tuberculosis and a biopsy from the sinuses is conclusive.
Penicillin is the drug of choice, but surgical excision of the sinuses might be required.
Footnotes
Contributors GR: concept, planning, literature search, manuscript writing, editing and final approval. SC: diagnostics, literature search, manuscript writing, editing and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.