Article Text

Abstract
Endoscopic biliary stenting is a well-recognised method of palliation of malignant biliary obstruction. Distal stent migration causing duodenal perforation is an uncommon complication of this procedure and is usually delayed. Early stent migration resulting in duodenal perforation is extremely rare and can be easily overlooked. We present a case of stent migration and resultant intraperitoneal duodenal perforation that occurred 24 hours following plastic stent insertion for a malignant biliary stricture in a 63-year-old woman. The patient required emergent abdominal laparoscopy with the placement of intraperitoneal drain, followed by endoscopic extraction of the stent and closure of the defect using a through-the-scope clip. This case report addresses intraperitoneal duodenal perforation secondary to early migration of biliary stents. Special emphasis is placed on the importance of prompt diagnosis and the use of endoclips in the management of this serious complication of endoprosthesis.
- Endoscopy
- Gastrointestinal Surgery
- Biliary Intervention
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Endoscopic biliary stenting is the preferred modality for palliation of malignant biliary obstruction. As compared with self-expandable metallic stents, plastic stents are less expensive but have a much higher risk of migration, both proximal and, more commonly, distal.1 In various studies, stent dislocation ranges between 5% and 14% of cases, with the migrated stent most frequently passing in the stools without complications.2 3 Approximately 1% of migrated stents causes intestinal perforation, most commonly in the duodenum.2 Retroperitoneal perforation caused by stent migration is more common than intraperitoneal perforation, but the latter is more serious.2 4 Most commonly, the perforation is delayed, occurring days to weeks after placement,3 but in rare cases, it can occur as early as 24 hours after stent insertion.5 6 The present report highlights the challenging setting of early stent-related intraperitoneal duodenal perforation and its management by means of minimally invasive laparoscopic surgery and endoscopic repair using through-the-scope clips (TTSC).
Case presentation
A previously healthy 63-year-old woman presented to our hospital with a 3-week history of painless jaundice. She also reported pruritus, anorexia and a 7 kg weight loss over a period of 8 weeks.
Liver function tests revealed total bilirubin 128.9 μmol/L (normal 5–21), direct bilirubin 118 μmol/L (normal <5), alkaline phosphatase 503 U/L (35–104), γ-glutamyltranspeptidase 1442 U/L (5–36), alanine aminotransaminase 310 U/L (0–33) and aspartate aminotransferase 211.1 U/L (0–32).
Abdominal ultrasound disclosed distended gall bladder with multiple tiny stones and sludge, whereas the biliary tree could not be visualised due to excessive gas. Endoscopic retrograde cholangiopancreatography showed intrahepatic biliary dilatation and common bile duct dilatation (maximum diameter 16 mm) with non-opacification of the distal portion (figure 1). Thus, brush cytology was obtained and a 10-French, 10 cm straight plastic stent (Biliary Stent (PE) SU, ENDO-FLEX, Germany) was inserted.
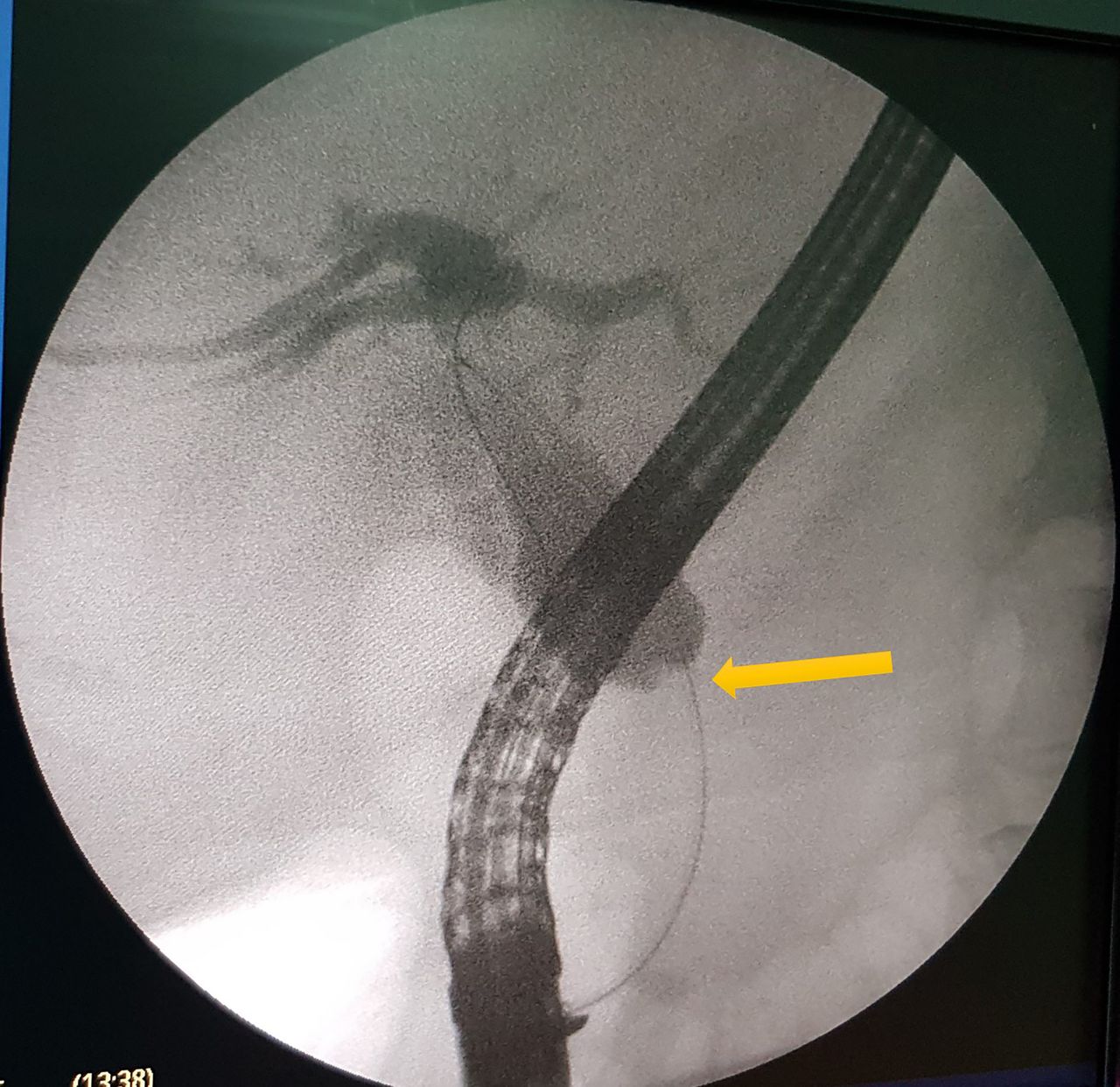
Cholangiography image showing dilatation of the intrahepatic and extrahepatic biliary tree with non-opacification of the distal common bile duct (yellow arrow).
Given the clinical suspicion for neoplastic aetiology of her common bile duct obstruction, a CT scan (pancreatico-biliary protocol) was performed and revealed a partially defined hypodense lesion in the head of the pancreas measuring about 1.4×1.5 cm with no associated lymphadenopathy or liver metastasis. The tumour marker CA 19.9 resulted high at 180.9 U/mL (normal 0–27). At that time, the patient declined any potential surgical intervention. Her next day liver function tests were remarkably improved, and she was discharged home with the recommendation to follow-up in 1 week for further discussion of her condition. However, 24 hours after her discharge, she developed severe, diffuse abdominal pain associated with nausea and vomiting. On arrival in our emergency room, her examination revealed a temperature of 38.2, blood pressure 110/70 mm Hg and heart rate 120/minute. She had diffuse abdominal tenderness to palpation with guarding and rigidity. Laboratory tests revealed leukocytosis (white cell count 20.7×109/L), whereas liver function tests showed improvement as compared with her prestenting values. Pancreatic enzymes were normal. Abdominal ultrasound showed abundant liquid in the peritoneal cavity.
Treatment
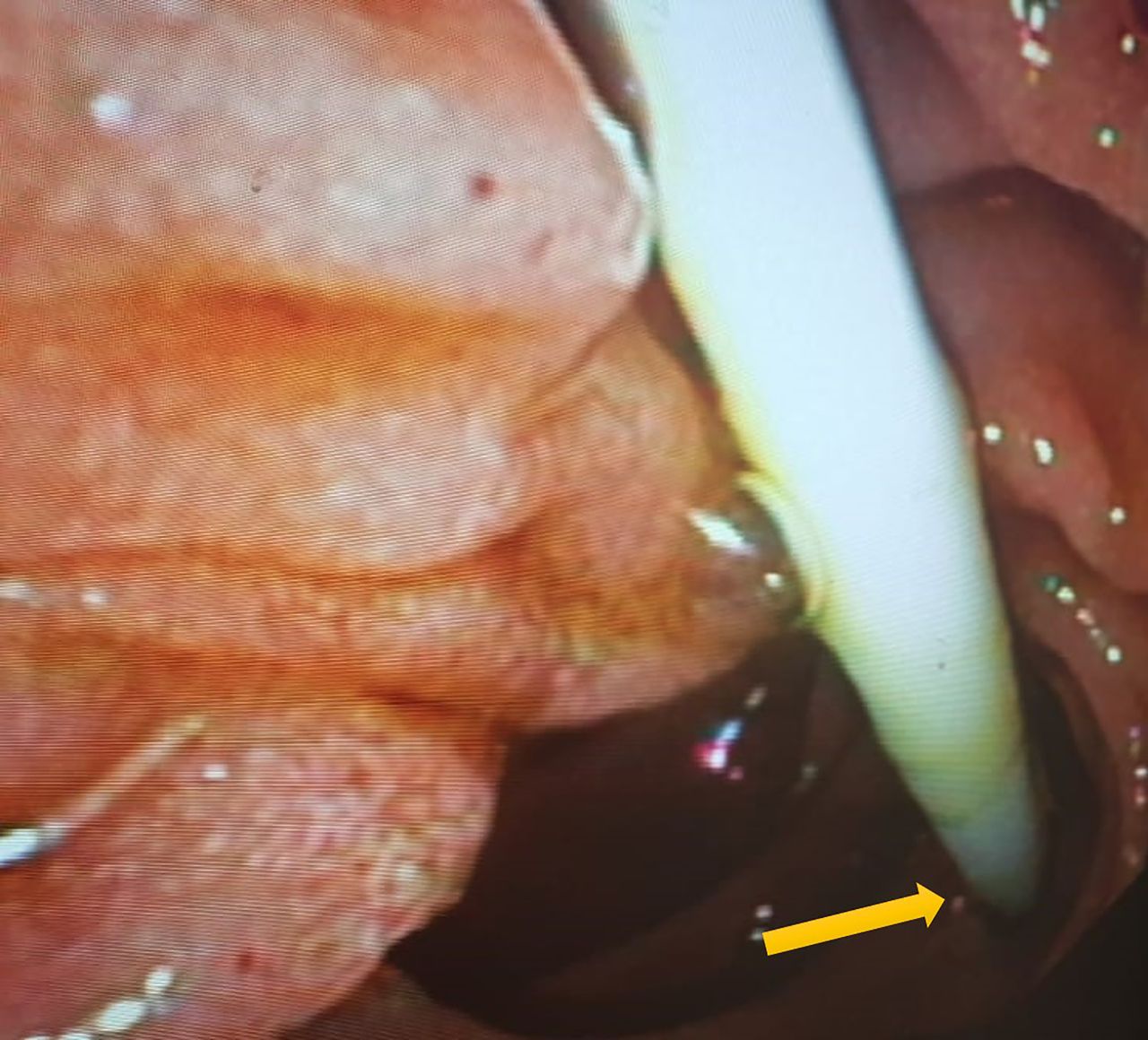
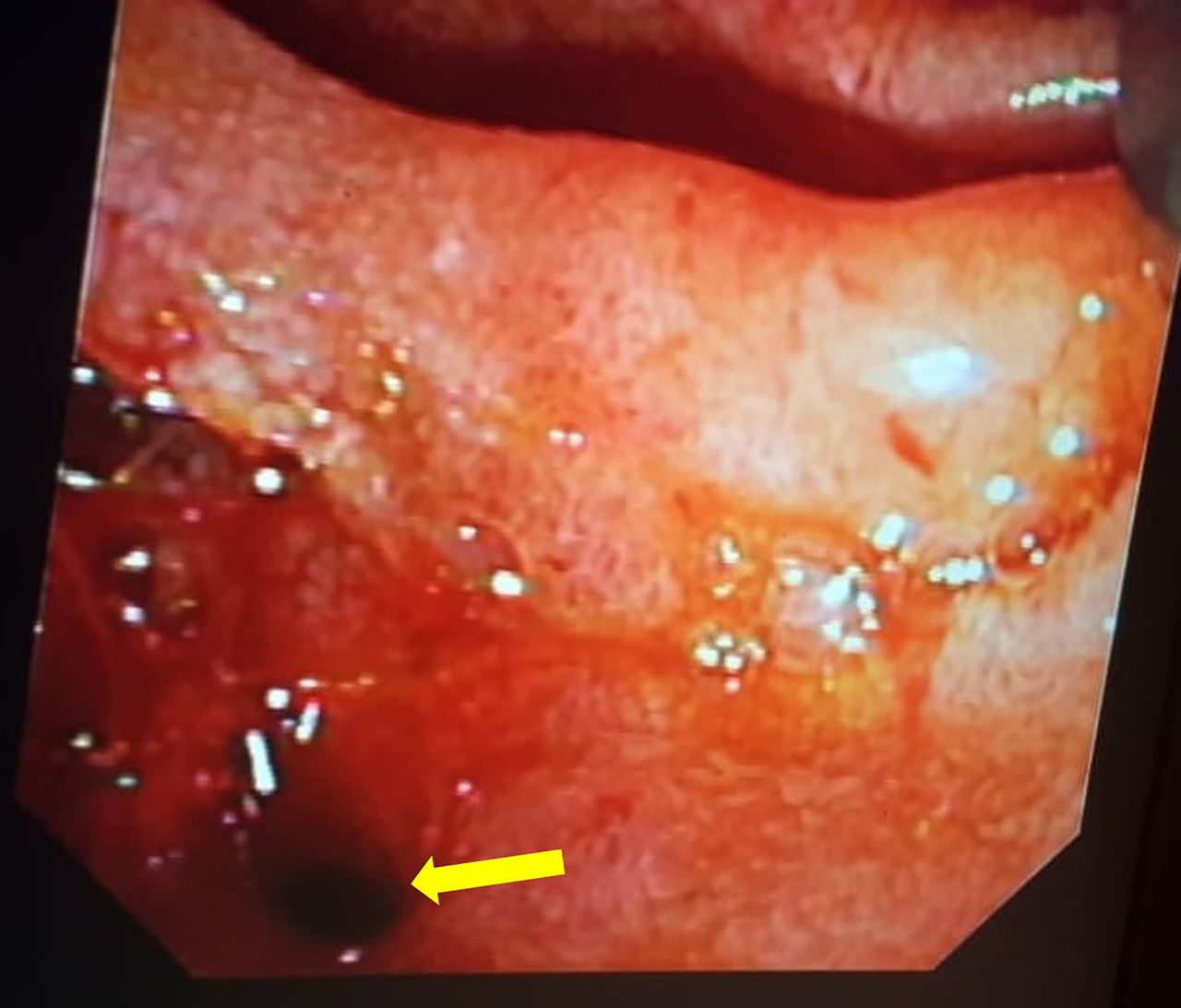
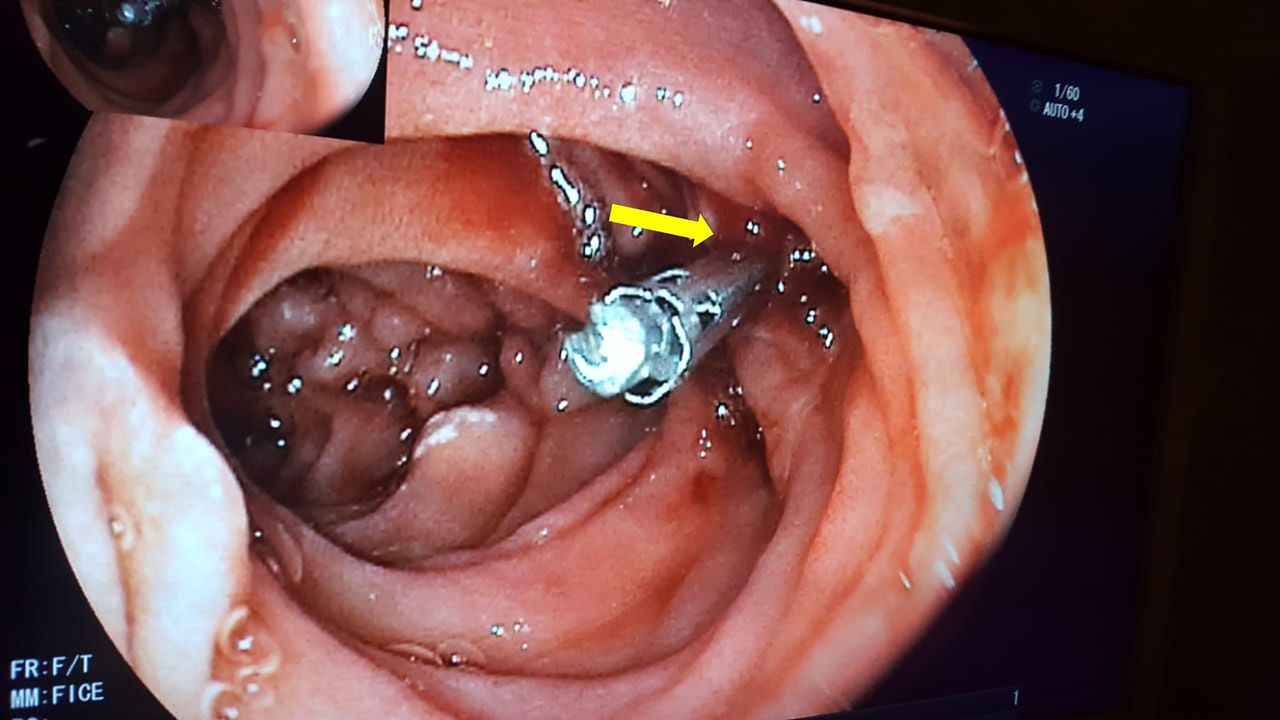
Because of the evidence of biliary peritonitis, emergent abdominal laparoscopy was carried out, yielding approximately 500 mL of turbid bile from the peritoneal cavity (figure 2). The abdominal cavity was washed out with normal saline and a drain was left in place. At that time, because of the intraoperative findings of bile in the peritoneal cavity which raised the question of duodenal perforation, contrast-enhanced CT of the abdomen was urgently arranged. Postlaparoscopy contrast-enhanced CT scan showed partially migrated stent with the distal end perforating the third portion of the duodenum and protruding into the peritoneal space (figure 3). Subsequent upper endoscopy revealed partial distal migration of the stent, with distal end perforating the inferior wall of the third portion of the duodenum (figure 4). Using a grasping device (Aligator Forceps, ENDO-FLEX, Germany), the proximal end was first removed, then the distal end was pulled and retrieved, unveiling a 0.4×0.4 cm transmural defect (figure 5). Following that, using the through-the-scope technique, one clip (SAFECLIP, Rotatable, Re-Openable, G FLEX, Belgium) was applied to close the duodenal defect (figure 6). A nasogastric tube was placed and intravenous fluids and broad-spectrum antibiotics were started.

Laparoscopic image disclosing bile in the peritoneal cavity.

Coronal contrast-enhanced abdominal CT revealing the distal end of the stent (yellow arrow) perforating the third portion of the duodenum and protruding into the peritoneal space.

Endoscopic view showing perforation of the third portion of the duodenum by the distal tip of the stent (yellow arrow).

Endoscopic view of duodenal perforation after retrieval of the stent (yellow arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Endoscopic view showing closure of duodenal defect with one through-the-scope clip (yellow arrow).
Outcome and follow-up
Over the next 24 hours, the patient remained afebrile and haemodynamically stable, with decreased leukocytosis and resolution of symptoms. The abdominal drain was removed on postoperative day 4 and the patient discharged home after agreeing to undergo Whipple’s procedure, which was carried out 3 weeks later. Her postoperative course was uneventful. At follow-up visits, the patient was doing well and her laboratory tests were all normalised.
Discussion
Although migration of plastic biliary stents is relatively common (up to 14%), only 1% of cases result in intestinal perforation, whereas the vast majority of migrated stents pass unnoticed in the stools.2 3 The duodenum is perforated more commonly than other parts of the gut due to its comparatively thin wall and retroperitoneal fixation. Pressure necrosis caused by the distal end of stent combined with a retained proximal portion in the common bile duct leads to perforation and possibly biliary peritonitis, like in our case. The vast majority of the reported duodenal perforations were retroperitoneal.4 7 Retroperitoneal perforations, particularly in case of small defects, can present with ill-defined symptoms or even be asymptomatic. Conversely, they can be complicated by the development of bilioma or abscess, manifesting with fever, abdominal pain or overt septic shock.7 Only a few cases of stent-related intraperitoneal duodenal perforations have been described in the literature.6 8 Intraperitoneal perforations usually carry a worse prognosis, especially in case of delayed diagnosis and consequent biliary peritonitis.6 Therefore, the emergency room evaluation of these patients should include an urgent plain abdominal radiogram or, if readily available, a CT scan without contrast, as suggested by several investigators.9 10 Unfortunately, in our case, radiological imaging was not performed in the emergency room and thus the exact diagnosis was initially overlooked.
Most of the reported cases were caused by delayed (weeks to months after placement) stent migration.3 11 Early migration causing duodenal perforation is extremely rare.5 7 In our case, the early occurrence of perforation can be contributed to three factors: (1) the use of a straight stent; (2) the excessive length of the stent and (3) the retention of the proximal end in the common bile duct (CBD), preventing the stent from adapting to duodenal peristalsis and thus increasing the pressure necrosis force on the duodenal wall. The length of the stent as a potential risk factor for migration has been investigated in several studies. In their retrospective study of the incidence and risk factors of biliary and pancreatic stent migration in 589 patients, Johanson et al found that the use of longer stents was a frequently reported potential cause, but only papillary stenosis was a statistically significant risk factor for biliary stent migration.3 Conversely, a more recent and larger retrospective study of the risk factors of biliary plastic stent migration revealed that longer stents are more frequently associated with distal migration, especially in benign biliary strictures.2 Therefore, we recommend the use of shorter, curved stents, which have been shown to be associated with lower rate of migration and/or consequent perforation.3 12 In our patient, intraperitoneal perforation occurred <24 hours after stent placement, leading to biliary peritonitis. To our knowledge, only one case of this combination (early and intraperitoneal) has been reported in the literature.6 Thus, clinicians should maintain a high index of suspicion to promptly recognise this serious complication of biliary stenting, irrespective of the time elapsed between stent placement and the onset of symptoms.
The decision to treat medically, surgically or endoscopically depends essentially on the general condition of the patient, site of injury (duodenum, small or large bowel), size and type of perforation (intraperitoneal or retroperitoneal), and the readiness of surgical and endoscopic expertise at the centre. Conservative management is suitable for stable patients with small intestinal wall defects in the absence of large fluid collections and/or peritonitis.12 13 In the present case, the perforation was associated with obvious signs of peritonitis. Therefore, emergent laparoscopy was needed to prevent further deterioration and complications such as infected collections and/or sepsis, despite the absence of an exact preoperative diagnosis.
The use of endoclips in the management of gastrointestinal perforations has been reported to be a valid alternative to the more invasive surgical intervention.7 14 The choice of the endoscopic technique is determined based on the size and anatomical location of perforation, and the endoscopist expertise available at the centre.14 Perforation size <1 cm with favourable location can be rather easily closed with ‘freehand’ TTSC.6 However, due to the narrow wingspan of the TTSC, multiple clips are usually needed for the repair. Additionally, there is some concern that the closure may not be complete as only the surface layer is grasped by the clip, unlike the over-the-scope clipping (OTSC) technique.14 15 Nevertheless, the use of TTSC is easier and faster to apply and widely available. Compared with the TTSC, the OTSC has higher retention force and enables capture of a larger tissue volume, in addition to the ability to close defects as large as 2 cm.14 16 Yet, OTSC is not widely available and has a long learning curve, due to its technical complexity.17 Therefore, the decision to use OTSC or TTSC should take into account the size of the perforation and the local endoscopist expertise.
In conclusion, duodenal perforation due to stent migration should be included in the differential diagnosis of patients presenting with unexplained abdominal pain after biliary stent insertion. The meticulous selection of stent length and shape is recommended to decrease the rate of biliary stent migration and consequent perforation. A high index of suspicion for perforation should be maintained when evaluating these patients, irrespective of the duration of stent placement. Minimally invasive laparoscopic surgery combined with endoscopic clipping is effective in decreasing morbidity and mortality. The use of TTSC to close duodenal wall defects is an effective and safe procedure and can obviate the need for more invasive surgical interventions. However, larger comparative studies of the efficacy and safety of TTSC and OTSC are needed.
Patient’s perspective
Initially I was reluctant to undergo curative surgery because of the inherent operative risk and my fear of post-operative pain, but later I changed my mind because of what I went through due to this nasty complication of biliary stenting. Actually I told my doctors that the pain I came back with due to inflammation of my abdomen was worse than any possible post-surgery pain.
Learning points
Intraperitoneal duodenal perforation is an important differential diagnosis in any patient with a plastic biliary stent presenting with signs of peritoneal irritation and/or fever.
Stent migration is usually delayed (weeks to months), but it can occur as early as 24 hours after stent insertion.
Plain abdominal radiographs or CT of the abdomen should be the initial diagnostic tool in patients with a biliary stent presenting with unexplained abdominal pain.
Closure of the duodenal wall defect with through-the-scope clips is effective and can obviate the need for the more invasive surgical repair.
Appropriate selection of the type and length of the stent should decrease the rate of migration and/or perforation.
Footnotes
Contributors KJ: designed this report, assisted in drafting the manuscript and critically revised the final version. BA and AS: searched the literature and wrote the first draft of the manuscript. ARA: assisted in designing the report and proofread the article. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.