Article Text

Statistics from Altmetric.com
- respiratory medicine
- general practice/family medicine
- pneumonia (infectious disease)
- lung cancer (oncology)
- radiology
Description
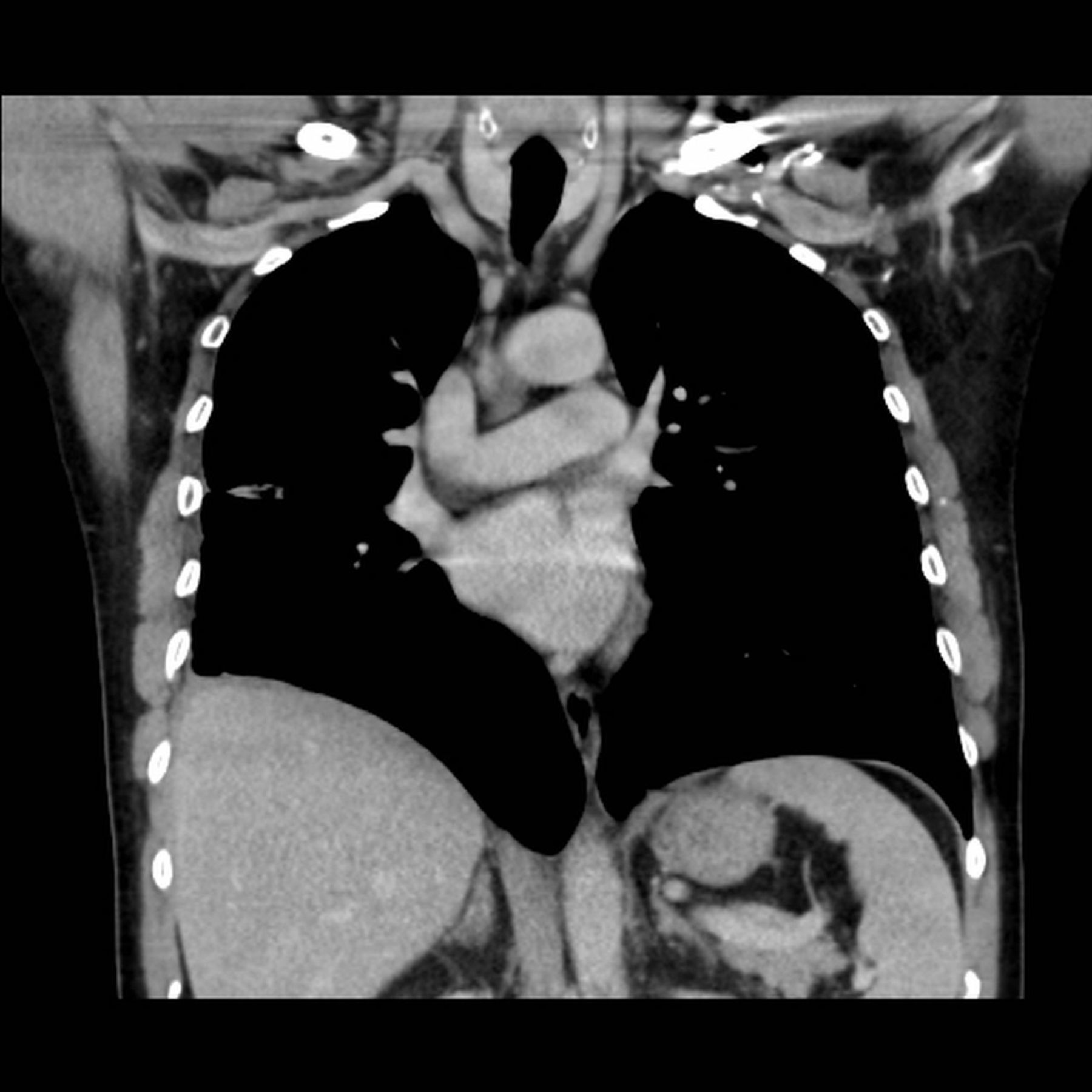
A 46-year-old man with a history of cough and night sweats extending over 4 weeks was admitted because of new-onset chest pain. Blood analysis highlighted elevated inflammatory markers. CT showed a spiculated lung mass, highly suspicious of malignancy (figure 1, arrow). Histopathology of bronchoscopy-guided transbronchial biopsies revealed no malignancy but giant cell granulomas around birefringent material (figure 2, arrow). On admission, the patient denied intravenous drug use. Despite antibiotic treatment with amoxicillin/clavulanic acid and clarithromycin, fever occurred after a week. CT evidenced abscessing pneumonia and empyema (figure 3, arrow). A chest tube was placed and antibiotics were switched to piperacillin–tazobactam for 2 weeks and clindamycin for 3 weeks, consecutively. The patient responded well to this treatment with a decrease of fever and chest pain, and normalisation of the inflammatory markers. Two months later, CT demonstrated complete resolution of the lung mass and empyema (figure 4). After all, the patient eventually admitted having repeatedly injected crushed morphine tablets dissolved in water. Accordingly, the initial findings of the CT scan and the lung biopsy were interpreted as pulmonary talcosis, a granulomatous disease of the lung caused by intravenous misuse of oral drugs. Injected material had embolised into the lung and had caused foreign body reaction (talc granulomatosis), mimicking lung cancer. Due to superinfection, empyema had evolved.

CT images showing spiculated mass in the right lung measuring 6, 6×4, 5×3, 9 cm with close contact to pleural space (arrow).
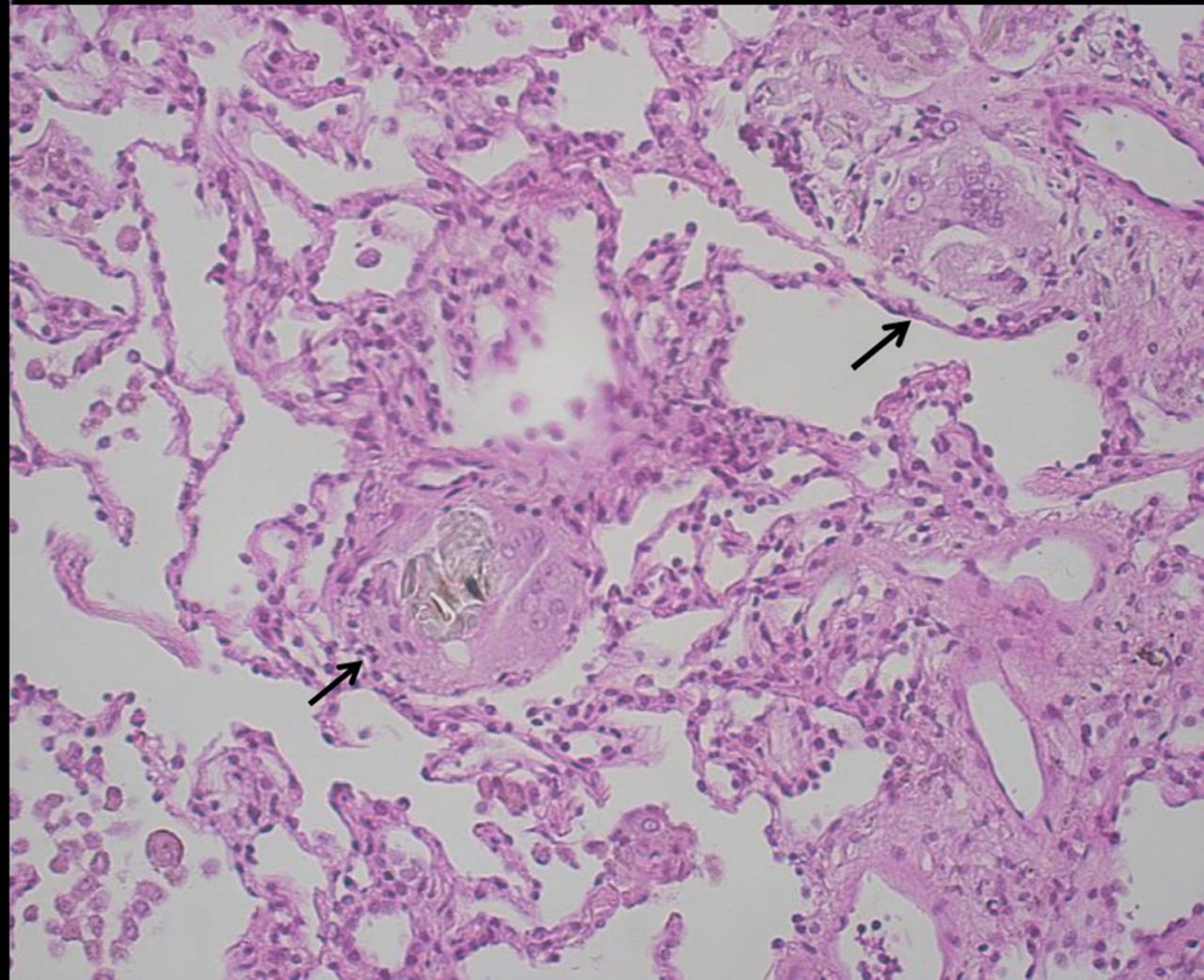
Transbronchial biopsies with no malignancy but vascular and interstitial giant cell granulomas around birefringent material (arrow).
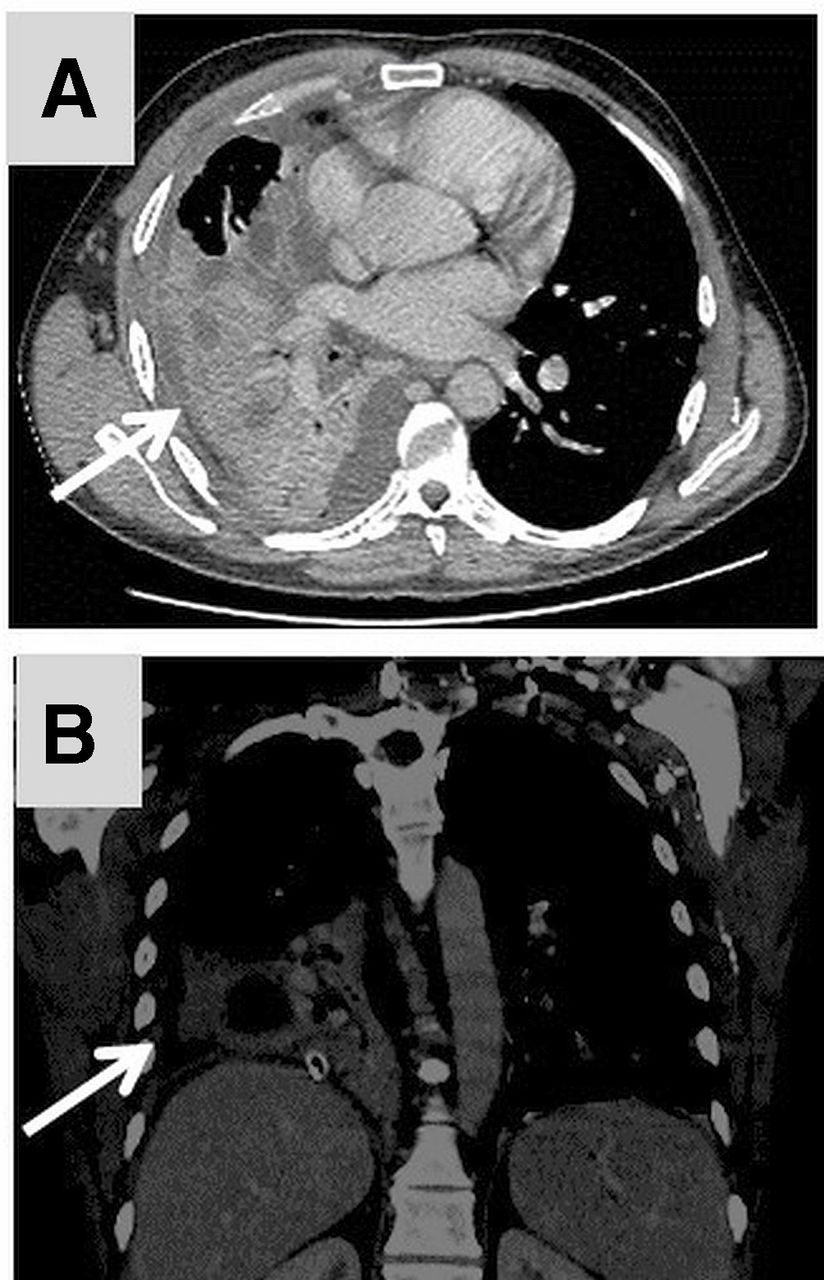
CT images demonstrating abscessing pneumonia and empyema (arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT images demonstrating complete resolution of the lung mass and empyema.
Pulmonary talc granulomatosis (or pulmonary talcosis) is a rare condition. In the past, it was the result of the inhalation of talc dust. In the 1960s, pulmonary talcosis emerged as a new phenomenon caused by intravenous injection of dissolved oral medication and at last by illegal drug abuse, such as cocaine.1 Frequently these drugs are elongated with talc to increase the mass and especially the costs. Talc (magnesium silicate) is a common bulking agent in oral medications. In drug users, who intravenously inject medications intended for oral use, small particles of talc reach the pulmonary vessels and can cause foreign body granulomatous reaction in the pulmonary interstitium.2 Foreign-body granulomatous reactions have also been described in other organs, such as liver, spleen, retina, kidney, skin, pancreas, lymph nodes and bone marrow.3
Because pulmonary talcosis has a very low incidence, the diagnosis can be a challenge. Talc can lead to interstitial fibrosis and in some cases to intravascular talcosis in the pulmonary arteries.4 5 In the present case, an extensive formation of pulmonary talcosis mimicked a neoplasia by forming a solitary lung mass, which is a rare feature.
Learning points
A malignancy is not always a malignancy.
Illegal drug abuse can make a lot of special and rare complications.
Sometimes you have to ask three or four times to get the right answer.
Footnotes
Contributors DS and CAR designed and directed the project, treated the patient, make the literature research, and wrote the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.