Article Text

Abstract
Surgical treatment of lipomas is typically only considered when they are painful or unsightly. We present the case of a massive hip lipoma; with this extreme case, we show that the global prolongation of life expectancy can lead to other indications of removal.
- general surgery
- plastic and reconstructive surgery
- dermatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Lipomas are benign and common soft-tissue tumours with many different clinical presentations. Surgical management can sometimes be tricky, and surgeons must keep in mind the potential risk of malignancy with large tumours.
Case presentation
We describe the case of a 90-year-old patient with a giant gluteal lipoma having evolved over more than 20 years. The patient was well aware of this slow-growing painless mass on his right hip but refused any treatment. He was addressed to our surgical consultation by his family doctor for lameness and unbalanced walking. (figure 1A, B).

(A) Posterior view of the patient’s lipoma. (B) Lateral view of the patient’s lipoma.
Investigations
Even though a benign lipoma was clearly suspected, a CT scan was performed. However, the lesion was so large that it could not be scanned entirely (figure 2). The tumour-like lipoma seemed to be in contact with the sacrum, the tuber ischiadicum and the greater trochanter. Furthermore, there was a suspicion of an infiltration of the flexor’s muscles of the right leg. Vascularisation of the lipoma was mainly provided by an enlarged superior gluteal artery.
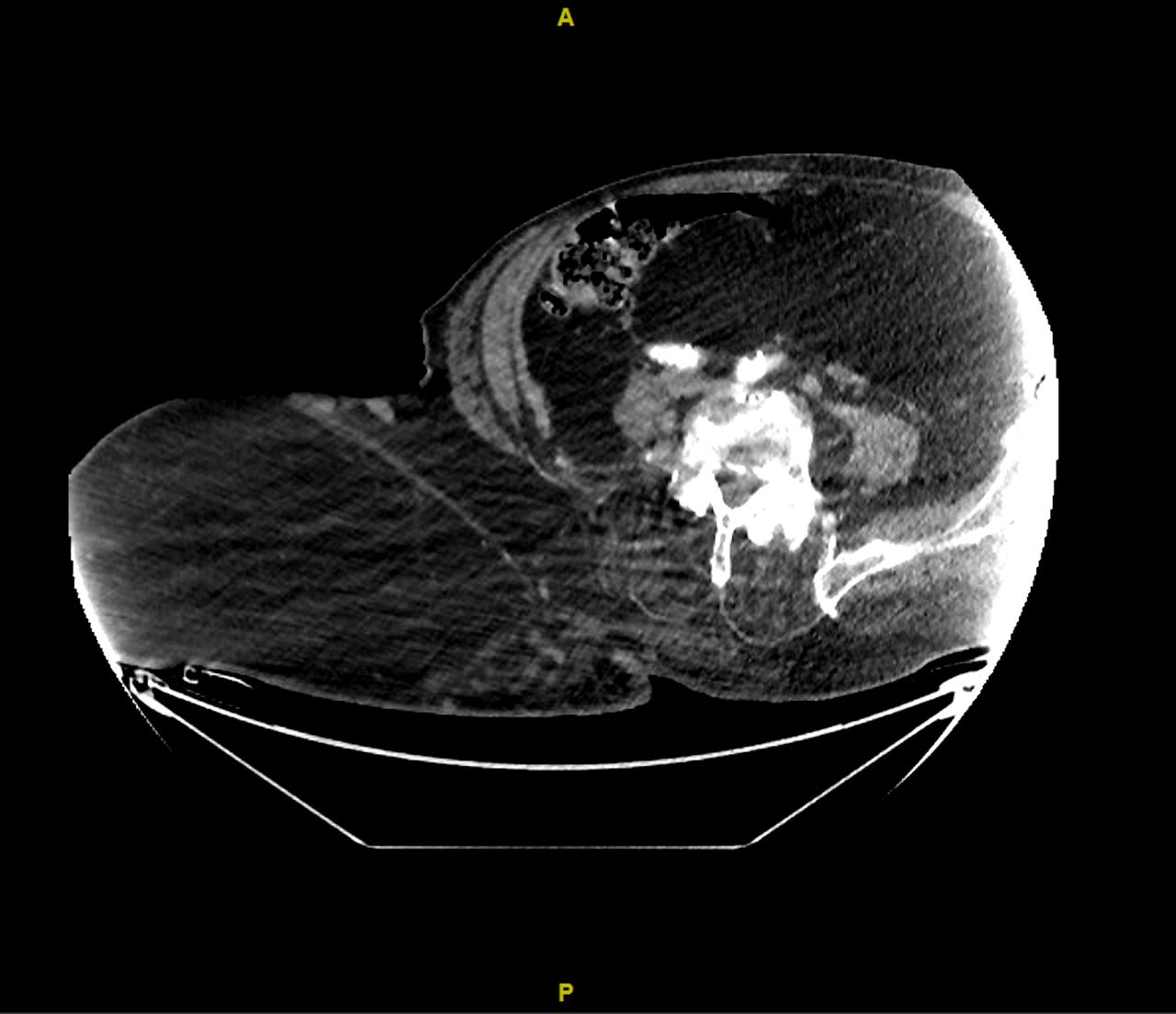
CT scan of the right hip lipoma.
Treatment
After discussing the pros and cons of an intervention with the patient and his family, the decision was taken to remove the mass surgically. The patient was installed in a dorsal decubitus position (figure 3A). The operation resulted in the removal of a 30×60 cm 20 kg lipoma (figure 3B).

{kind=link}
{kind=link}
{kind=link}
(A) Dorsal decubitus surgical position. (B) Lipoma total dissection.
Outcome and follow-up
The pathology report confirmed that the tumour was benign. Skin was preserved in order to allow a functional reconstruction of the gluteal region. Wound management was simple, and follow-up was unremarkable. Additionally, the patient received intensive physiotherapy for walk recovery and after 5 weeks he could achieve completely independent walking.
Discussion
What makes this case interesting is the fact that even a benign pathology such as a lipoma progressed into a situation requiring delicate surgical management, both due to the technical aspect of the operation itself, and because of the patient’s advanced age.
With no difference in prevalence across genders and a 40–60 years old average age,1 lipomas are the most frequent benign soft-tissue tumours. Whether isolated or multiple, congenital or post-traumatic,2 lipomas are frequent in our daily routine; some studies mention the genetic implication in more than 50% of them.3 Even with minimal risk of malignant evolution, the first step of imaging should be ultrasonography,4 sometimes associated with MRI for large or deep tumours.5 Various treatments can be suggested for mechanical or aesthetic concerns. Surgery is the most appropriate treatment, associated with other techniques6 (suction, soft-tissue reconstruction, flap and so on).
Various pathologies imitating lipomas, such as lipomatosis or lipodystrophy, should be distinguished from it.7 The WHO gives a standard classification for all types of lipomas.8
Giant lipomas are a specific entity as their precise definition is only based on the general aspect of the tumour, with a specific size and weight cut-off given by Sanchez et al.9 In order for a lipoma to be called ‘giant’, the lesion must be at least 10 cm in one dimension or weigh a minimum of 1 kg. Based on recent literature, the case we report here is the second largest sub-cutaneous lipoma ever described (table 1).
Largest giant lipomas in French/English-language literature (>10 cm and >1000 g)
Learning points
Giant lipomas are above all aesthetics concerns but in advanced form a functional problem.
Benign tumours with low risk of malignant evolution.
Surgery as if aesthetic or functional disorders.
The transformation of a large lipoma (>10 cm) to a liposarcoma is rare.
References
Footnotes
Contributors AL wrote the article; MM, FC and BE verified the analytical methods and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.