Article Text

Statistics from Altmetric.com
Description
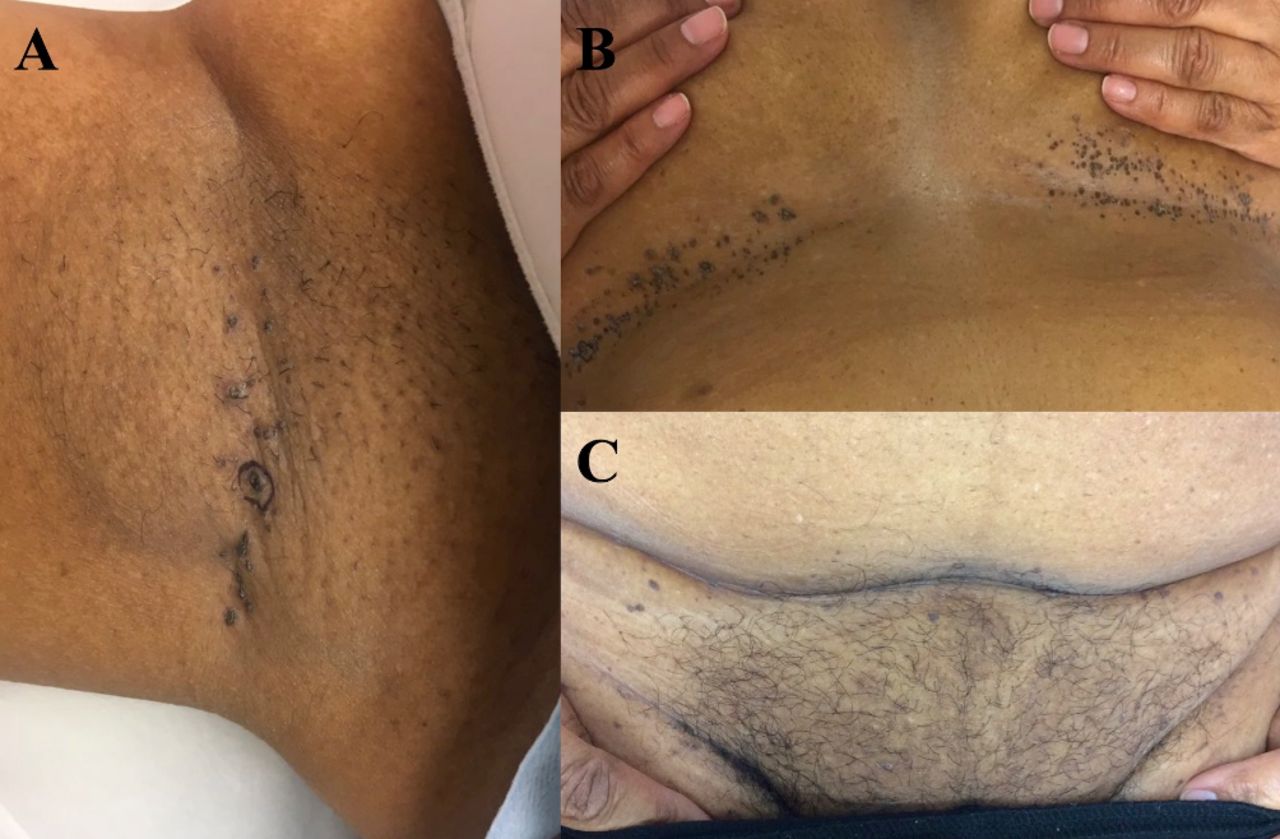
An otherwise healthy 69-year-old woman presented with a several months’ history of a pruritic eruption in intertriginous areas. No treatments had been tried, although the patient had used antiperspirant for years and recently switched to a new brand. Physical exam showed linear hyperpigmented and hyperkeratotic papules in the right axilla, bilateral inframammary folds, and infrapannus and inguinal folds (figure 1). The differential diagnoses included Hailey-Hailey disease, Darier disease, Fox-Fordyce disease and pemphigus vegetans.

Linear hyperpigmented and hyperkeratotic papules in the (A) right axilla, (B) bilateral inframammary folds, and (C) infrapannus and inguinal folds.
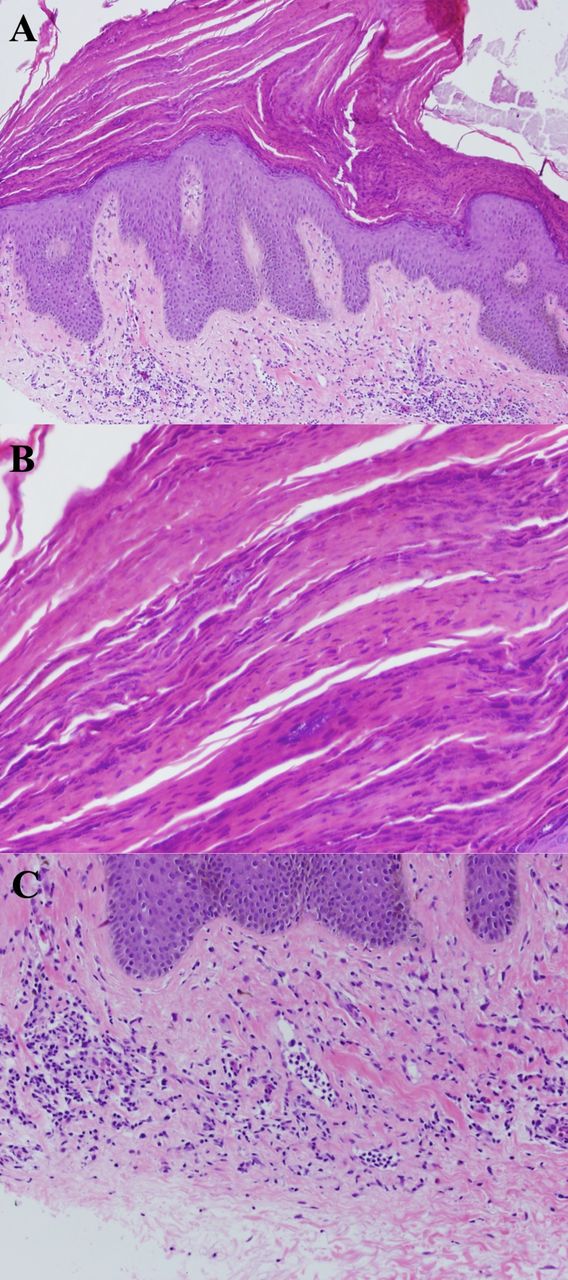
Punch biopsies were obtained from the right axilla and inframammary area. Histology revealed psoriasiform hyperplasia, retained keratohyalin granules within a thickened stratum corneum and a superficial lymphohistiocytic inflammatory infiltrate (figure 2). Bacterial and fungal cultures were negative. The patient was subsequently diagnosed with granular parakeratosis. Following 2 weeks of treatment with hydrocortisone 2.5% ointment and antiperspirant avoidance, her disease resolved (figure 3); the patient’s lesions ‘fell off’ when she cleaned herself with a towel.

(A) Psoriasiform hyperplasia. H&E 10× (100× original magnification). (B) Retained keratohyalin granules within a thickened stratum corneum. H&E 40× (400× original magnification). (C) Superficial lymphohistiocytic inflammatory infiltrate with scattered eosinophils. H&E 20× (200× original magnification).

{kind=link}
{kind=link}
{kind=link}
Right axilla: lesions resolved.
Granular parakeratosis is an idiopathic and benign skin disease with an incidence of approximately 0.005%.1 It was first described in 1991 with a case series of four patients with granular parakeratosis involving the axilla.2 Since the initial case series, additional cases of granular parakeratosis have been described,3–8 including several with involvement of multiple intertriginous sites.9 10
Granular parakeratosis tends to affect women older than 40 years but has been described in both sexes and a range of ages.11 Patients classically present with a shorter than 1-year duration of eruptive red to brown hyperkeratotic papules and plaques in intertriginous areas that can be asymptomatic, pruritic or painful.1 11 Involvement can be unilateral or bilateral.11 Relevant differential diagnoses include Hailey-Hailey disease, Darier disease, Dowling-Degos disease, pemphigus vegetans, intertrigo, dermatophytosis and candida.11
Histopathology is pathognomonic for granular parakeratosis. Classically, the epidermis is acanthotic or psoriasiform with hyperkeratosis, parakeratosis and retention of keratohyalin granules in the stratum corneum.1 11 This constellation of findings has been described incidentally in a variety of diseases, from molluscum contagiosum to dermatomyositis, leading to the notion that granular parakeratosis represents a histological reaction pattern rather than a distinct clinical disease.11
Several theories exist regarding the pathogenesis of granular parakeratosis. One theory hypothesises that a contact allergy to deodorants and antiperspirants disrupts the breakdown of profilaggrin to filaggrin.2 Additionally, moisture and friction within intertriginous areas may result in irritant contact dermatitis, causing the skin to thicken as a protective mechanism.11 Lastly, it is possible that granular parakeratosis represents a distinct and inherent disorder of cornification.11
The treatments for granular parakeratosis are varied. Fortunately, the disease is often self-limiting.11 Treatments used with success in published case reports include topical treatment with corticosteroids, vitamin D analogues, retinoids, antifungal agents and ammonium lactate; oral treatment with retinoids, antibiotics and antifungal agents; and procedural treatment with cryotherapy and botulinum toxin injection.11 12
Granular parakeratosis is a rare disorder characterised by hyperkeratosis, parakeratosis and retention of keratohyalin granules in the stratum corneum. Herein, we report a case of granular parakeratosis with multiple site involvement.
Learning points
Granular parakeratosis is a rare skin disorder with characteristic histopathological findings.
Granular parakeratosis can involve multiple intertriginous areas.
Footnotes
Contributors AJZ: design, drafting and revision. MLC: patient care, design, informed consent, drafting and revision. AMG: patient care, conception, design, drafting and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.