Article Text

Abstract
A 28-year-old man previously diagnosed and treated for testicular sex cord-stromal tumour (TSCST) presented with symptoms of fever, night sweats and fatigue. Following initial investigations for an infectious aetiology, imaging studies detected two large liver lesions. Histopathological assessment of the tumours revealed that they were metastases from the TSCST for which the patient had radical inguinal orchiectomy and retroperitoneal lymph node dissection 5 years prior. The curative-intent management of the bilobar liver metastases necessitated staged resection due to the chemoresistant and radioresistant properties of TSCST. The size of the lesions was such that procedures to induce rapid liver hypertrophy were required between surgeries. Both liver metastases were successfully removed following this approach. The patient remains recurrence-free 1 year after surgery and has maintained predisease levels of performance. Nevertheless, he continues to be followed for routine CT scans at regular intervals.
- cancer intervention
- surgical oncology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Testicular sex cord-stromal tumours (TSCST) are rare, accounting for less than 5% of all testicular neoplasms.1 Approximately 10% of TSCST are malignant, and most cases of metastasis develop within the first 2 years after initial diagnosis.2 3 The retroperitoneal lymph nodes are the most frequent site of metastatic disease, though metastases to the liver, lung and bone are not uncommon.2–4 Treatment options for TSCST are rather limited because neither chemotherapy nor radiotherapy have been effective. Therefore, the therapeutic approach for malignant TSCST has traditionally consisted of radical inguinal orchiectomy followed by retroperitoneal lymph node dissection (RPLND).3 5 6 Still, the prognosis for metastatic TSCST remains quite poor due largely to rapid disease progression and to the lack of available treatments. For this reason, radiographic surveillance is important for patients with multiple pathological risk factors associated with malignancy.5 6
We report a case of bilateral liver metastases from a TSCST in a 28-year-old man, occurring 5 years after the performance of radical inguinal orchiectomy and RPLND.
Case presentation
A 28-year-old man was admitted to the infectious diseases clinic with a 3-week history of fever, night sweats and fatigue.
A thorough travel history was taken, in which the only notable information was that the patient had encountered at least one individual with tuberculosis within the previous year.
His medical history included an upper respiratory tract infection and persistent cough 6 weeks prior to admission. Furthermore, the patient was treated for testicular cancer at the age of 23 years. He underwent a right radical inguinal orchiectomy, and histopathological evaluation of the mass determined that it was an unclassified sex cord-stromal tumour. The diagnosis was made on the basis of morphological and immunohistochemical findings, including: trabecular and cord-like arrangement, prominent cytoplasmic vacuoles, nuclear grooves, positive stains for inhibin and vimentin and negative stains for alpha-fetoprotein, cytokeratin AE1/AE3, c-kit and placental alkaline phosphatase. He subsequently had aortic lymph node dissection and follow-up CT scans of the abdomen and pelvis. There was no evidence of metastatic disease in the lymph nodes that were removed, nor in the scans of the abdomen and pelvis. Thereafter, the patient was followed every 6 months for blood tests and chest X-rays.
Investigations
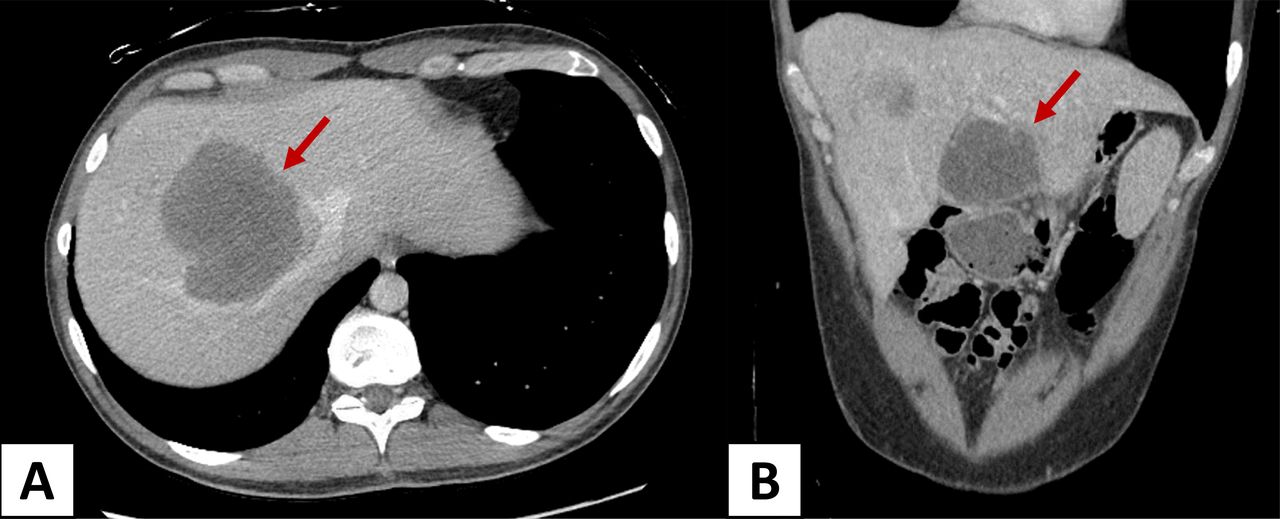
Laboratory tests revealed mildly elevated liver enzymes and mild anaemia. Multiple serologies and blood smears were performed to rule out a variety of infectious diseases, all of which were negative. Nevertheless, a positive monospot test was eventually obtained several weeks into the investigations. Based on these initial findings, the patient was suspected of having slowly resolving cases of infectious mononucleosis and hepatitis. However, imaging studies ultimately revealed two large liver lesions—one in segment III, and the other involving segments V, VII and VIII (figure 1A,B). These were biopsied and histopathologically confirmed to be liver metastases from the TSCST. An 18F-fluorodeoxyglucose positron emission tomography-CT scan was later performed to exclude extra-hepatic disease. In addition to the two known liver lesions, two areas of uptake were identified in the hilum of the liver and in the right chest wall; both were biopsied and neither revealed evidence of metastatic disease.

CT scans showing bilateral liver metastases: (A) right-sided lesion (B) segment III lesion.
Treatment
After having consulted with hepatobiliary surgeons, medical oncologists, pathologists, radiologists and urologists at our institution through multidisciplinary meetings, as well as with hepatobiliary surgeons at other high-volume centres, it was decided that the best outcome would be achieved by resecting the two liver metastases because there were no effective chemotherapeutic agents for TSCST. Due to the bilateral configuration of the lesions, a staged resection was planned with curative intent. A detailed description of our staged hepatectomy strategy has previously been reported.7
Segment III, which contained a 6.5 cm lesion, was removed once an enlarged hilar lymph node was determined to be negative for neoplastic disease; this constituted the first stage of the planned resection. Portal vein embolisation (PVE) of the right anterior and posterior branches was performed postoperatively to promote the growth of the left liver remnant for the coming resection of the right liver mass.
However, PVE failed to induce sufficient liver growth on the left side to obtain a future liver remnant (FLR) that was considered adequate to sustain life; FLR was calculated as the ratio of remnant liver volume to total functional liver volume, with vessel and tumour volumes being excluded from the latter. Consequently, the associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) procedure was performed as a second stage to resect the remaining lesion. This ALPPS procedure included a partial transection along the line between segment IV and left lateral liver where the ensuing resection would be performed, and placement of an Amplatzer plug to occlude blood flow to the right lobe of the liver. The FLR increased from 19% to 29% over a period of 3 weeks (figure 2), allowing for the removal of the second lesion, measuring 9.8×9.2 cm, via right trisegmentectomy.

Measurement of the future liver remnant (yellow) prior to right trisegmentectomy.
Outcome and follow-up
The patient’s postoperative course was first complicated by a bile leak that was seen on an endoscopic retrograde cholangiopancreatography to be from the stump of the right hepatic duct. This was successfully managed with a plastic stent across the area of the leak. The patient also developed an abscess at the surgical bed which was initially well treated by the drain that had been inserted during the surgery, though it required a singular instance of repositioning by interventional radiology to improve drainage. He was discharged with the drain, which was later removed in an outpatient setting. However, the patient presented to the emergency department with fever and a rising white blood cell count several days following the removal of the drain. A CT scan revealed persistence of the abscess cavity, which was then managed by intravenous antibiotics and the insertion of a new percutaneous drain. A follow-up scan showed that the cavity had been significantly reduced, the drain was removed and the patient was discharged from the hospital.
The patient has since been followed in the outpatient clinic, with his initial CT scans at 3 months showing complete resolution of the abscess cavity. The most recent CT scans of his chest, abdomen and pelvis that were done 1 year after the surgery showed no evidence of disease recurrence (figure 3A,B). He is now back at work and has maintained predisease performance levels.

{kind=link}
{kind=link}
{kind=link}
One-year follow-up CT scans showing no evidence of disease recurrence: (A) left hepatic vein (B) main portal vein.
Discussion
In this case, we describe the diagnosis and management of bilateral liver metastases from a TSCST for which the patient had been treated over 5 years prior. The patient presented with fever, night sweats and fatigue, which prompted initial investigations for an infectious aetiology. Unexpectedly, however, two remarkable liver lesions were identified on imaging, and upon the pathological confirmation of their sex cord-stromal tumour origin, surgical resection was determined to be the only approach with curative intent.
TSCST are a rare type of cancer, and they are not as well documented as the germ cell tumours that account for the vast majority of testicular malignancies. Unlike these seminomas and nonseminomatous germ cell tumours, whose susceptibility to bleomycin, etoposide and cisplatin has led to substantial improvements in cure rates, TSCST are unresponsive to chemotherapy.8 The surgical management of local and metastatic TSCST, which includes radical inguinal orchiectomy and RPLND, is therefore paramount.
Other cases of metastatic disease being discovered many years following the removal of a TSCST via radical inguinal orchiectomy have been reported. Maeda et al described a patient with retroperitoneal lymph node metastasis 9 years after radical inguinal orchiectomy for a Leydig cell tumour, and Adayener et al described a patient with retroperitoneal lymph node metastasis 8 years after radical inguinal orchiectomy for a Sertoli cell tumour. In both cases, the patients underwent curative-intent RPLND.9 10 The current case is comparatively unique in that the patient developed metastases in a distant organ 5 years after having undergone radical inguinal orchiectomy and RPLND for an unclassified TSCST. The three notable elements that distinguish this case from previous reports of late metastasis from TSCST are: the peculiarity of the primary tumour’s histological classification, the delayed onset of metastatic disease in spite of preventative RPLND, and the location of the metastases. Furthermore, there are no documented cases of metastatic TSCST that discuss the management of metastases that developed in the liver.
Currently, there are no guidelines for the follow-up of TSCST patients after radical inguinal orchiectomy and RPLND. Biannual blood tests and chest X-rays were deemed to constitute adequate follow-up because RPLND was thought to have been curative given the absence of detectable nodal disease. The finding in the present case poses the question as to whether routine CT examinations of the abdomen and pelvis should be performed for post-treatment surveillance of TSCST.
Learning points
Extensive metastatic disease of the liver can present with non-specific symptoms resembling those that manifest in various infectious diseases.
Testicular sex cord-stromal tumours can give rise to distant metastases many years following radical inguinal orchiectomy and retroperitoneal lymph node dissection. Therefore, it is important to continue monitoring these patients periodically via imaging studies.
If possible, the surgical resection of testicular sex cord-stromal tumour metastases should be considered because they do not respond to chemotherapy or radiotherapy.
Footnotes
Contributors VP contributed to the literature research and writing of the manuscript. HA-M was a treating physician involved in the interpretation of data and revision of the manuscript. PM was a treating physician who contributed to the revision of the manuscript and provided general supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Obtained.