Article Text

Abstract
This case report describes a patient with complicated Crohn’s disease who presented to a routine gastroenterology clinic complaining of increasing white discharge from a chronic perianal abscess. MRI of the perineum established the diagnosis of a seminal vesicle fistula connecting to the perianal skin. He was treated conservatively, with optimisation of his Crohn’s disease medication regime. Seminal vesicle fistulation is a rare pathology.
- Crohn's disease
- radiology
- gastrointestinal surgery
- general surgery
- inflammatory bowel disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
There is a paucity of literature specific to this pathology. Case reports are therefore required for our better understanding and implementation of appropriate management strategies.
Case presentation
A 66-year-old man with complex Crohn’s disease, diagnosed at age 32, attended gastroenterology clinic for routine review in November 2017. He had a medical history of gastro-oesophageal reflux. Previous surgical intervention included a right hemicolectomy with terminal ileal resection and synchronous proximal jejunal resection at age 40. This was complicated by psoas abscess requiring repeat laparotomy, washout and drain insertion.
At clinic review, he had a symptomatic colovesical fistula, which was initially diagnosed at age 54, two perianal fistulae, initially diagnosed at age 61, and an intermittent enterocutaneous fistula in the right iliac fossa at a previous drain site. He also had chronic anal canal stenosis, requiring anal dilatation in the past. While he remained intermittently symptomatic from the fistulae at clinic, there were no complications requiring hospital admission and his symptoms were medically managed as an outpatient with full patient compliance.
His medications included azathioprine 50 mg three times per day, alendronic acid 70 mg once weekly, calcium carbonate and colicalciferol D3 tablets two times per day, lansoprazole 15 mg once daily and hydroxocobalamin injections every 12 weeks.
At the time of surgical clinic review, he had received his second infusion of infliximab. His main complaints at clinic were worsening of symptoms relating to his fistulae. Specifically, he complained of increasing white coloured discharge leaking from a perianal abscess.
Investigations
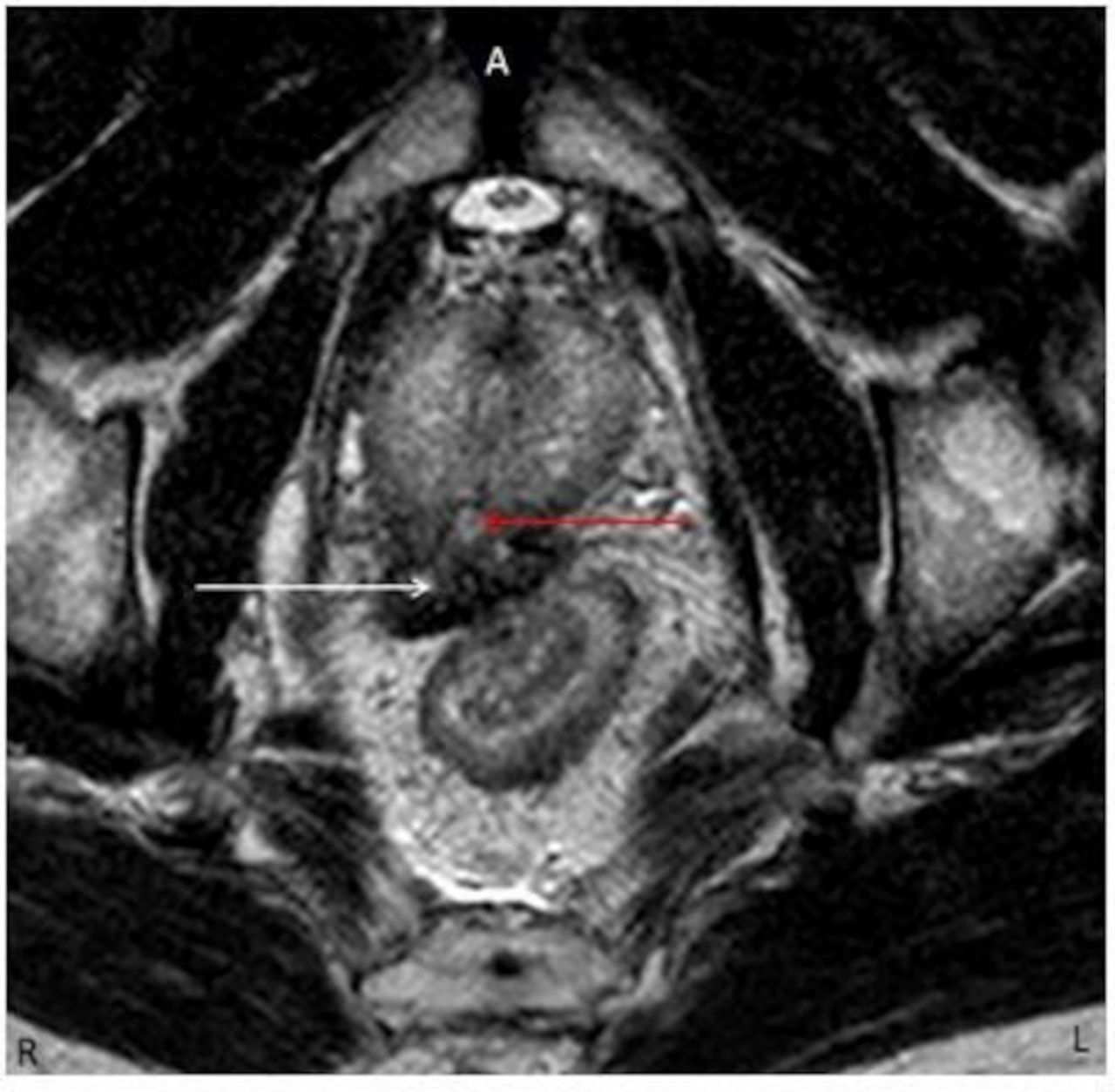
MRI of the perineum confirmed the culprit pathology (figure 1). Multiplanar (axial, sagittal and coronal) imaging was obtained using primarily T2-weighted turbo spin echo and short tau inversion recovery sequences; both these sequences are highly sensitive for fluid, which shows as high signal. Small field of view high spatial resolution (3 mm slice thickness) imaging was performed, giving precise anatomical characterisation. MRI revealed complex supra and extrasphincteric perianal fistulous disease with bilateral chronic tracts showing ongoing activity (figure 1).

Axial small field of view T2-weighted turbo spin echo (TSE) MRI of the perineum. Right-sided and left-sided perianal fistulous tracts (red arrows). High signal within denotes fluid consistent with active tracts. Low signal surrounding the tracts is fibrosis consistent with chronicity. A, anterior; L, left; R,right.
The right fistulous tract opened at 9 o’clock on the right buttock, 1.5 cm distal to the anal verge. It ascended the ischioanal/ischiorectal fat at 8 o’clock and crossed the levator plate superiorly (figure 2). Here it communicated with the distal rectum at 8 o’clock. The tract continued anterosuperiorly and terminated at the medial aspect of the right seminal vesicle (SV) (figure 3).

Coronal small field of view T2-weighted turbo spin echo MRI of the perineum. The right-sided fistula (red arrows) ascends in the ischiorectal fat passing through the levator ani (white arrow). L, left; R, right; Re, rectum.
Axial small field of view T2-weighted turbo spin echo MRI shows the most superior extent of the right-sided fistula (red arrow) ending at the medial aspect of the right seminal vesicle (white arrow).
On the left, the tract ascended the ischioanal/ischiorectal fat in the 3 o’clock position, piercing the puborectalis muscle and communicating with the distal rectum at 3 o’clock. From here, the tract continued posterosuperiorly terminating behind the distal rectum.
CT enterography (2 L of oral Klean prep over 1 hour followed by a contrast-enhanced acquisition timed at 45 s post injection) was performed to delineate the extent of active small bowel disease. The patient had a previous ileocaecal resection. There was active disease of the neoterminal ileum (nTI) with mural thickening (figure 4), hyperenhancement and mesenteric hyperaemia. Posteromedial to this inflamed segment was an ileocolic fistulous tract involving the nTI and colonic stump. There were several skip lesions elsewhere (not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Multiplanar reconstruction of CT enterography shows active disease of the neoterminal ileum (red arrow) with mucosal hyperenhancement, mural thickening and engorged vasa recta of the adjacent mesentery known as the ‘comb sign’ (white arrow). A, anterior; P, posterior.
Treatment
A multidisciplinary approach involving patient preference, gastroenterology and specialist colorectal surgical teams was required to decide on an optimum management strategy. The patient’s primary symptoms were owing to his perianal fistulae rather than anal canal stenosis. Both surgical and medical management options were discussed with the patient.
Surgical options were weighed up in terms of risk versus benefit for the patient, keeping in mind his relative lack of significant symptoms or infections. As well as the general risks of an operation such as bleeding and infection, there were patient-specific risks to consider. Due to the patients active Crohn’s disease, there was an increased risk of poor wound healing and chronic wound infection. Surgery could have made symptoms worse, caused further fistulae or abscess formation and resulted in pain (acute and chronic). Overall, the risks of surgery outweighed the benefits for him.
The patient continued to have active disease despite taking azathioprine. This was evident with increasing symptoms from his perianal disease and a rising faecal calprotectin. A colonoscopy in December 2015 showed no macroscopic disease of the rectum. An MRI of the perineum was performed in December 2016 showing active perianal fistulae but no occult or drainable collections. Thus, he qualified for a period of biologic therapy.
Infliximab has been shown to improve fistulae caused by Crohn’s disease. Infliximab may improve anal canal stenosis secondary to acute inflammation but is unlikely to improve chronic, fibrotic anal canal stenosis. Chronic anal canal stenosis can be treated with either balloon dilatation of the stenosis or with a more traditional ‘digital stretch’. In our patient’s case, given the chronicity of his disease, the infliximab was less likely to help and he previously had successful treatment with dilatation. At this point in time, the patient remained symptom free from his anal canal stenosis and so the main goal of treatment was to improve symptoms pertaining to his fistulae.
A conservative approach was chosen, maximising medical management in view of eliminating any ongoing inflammation. A period of observation while continuing on infliximab was the preferred treatment option for both the patient and the treating teams.
Outcome and follow-up
The patient attended 4 monthly gastroenterology clinics to assess the need for ongoing biologic treatment. After continuing on infliximab, the patient reported a significant improvement in symptoms. Primarily, that the leakage from the perianal fistulae had completely dried up.
He underwent an MR enterography scan to assess whether infliximab was helping with his small bowel fistulating disease, but there was no significant change from his previous imaging. He did not have a repeat MR of the perineum as he no longer had any symptoms from his perianal fistulae.
Discussion
Seminal vesicle fistulation (SVF) is a rare pathology.1 The literature is sparse; thus, case reports are imperative for allowing prospective case series. Crohn’s disease, previous surgery, diverticulitis, trauma and neoplasia have been implicated in its aetiology.1–4
Patient symptoms vary. Pneumaturia, testicular pain, rectal drainage, malodorous semen, decline in semen volume and fever have all been described as presenting symptoms in SVF.2–5 Chronic urinary tract infections not amenable to antibiotic therapy should also alert the clinician to the possibility of an SVT.5
Diagnostic imaging modality varies throughout the literature. In this case, MRI of the perineum was the investigation of choice, as it best depicts the soft tissue structures within the perineum as well as the fistulous tract(s).
MRI with concomitant vesiculography has been reported as a successful imaging modality when ejaculate volume is low.1 Alternatively, when the seminal vesicle is fistulating with bowel, CT of the abdomen and pelvis with both intravenous and rectal contrast has been shown to provide an accurate picture.2
Management options vary. Given the paucity of evidence, there is no gold standard approach. Principal treatment strategies are similar to that for other fistulae. Aetiology plays an important role. For example, if the fistula has formed secondary to an acute complication of diverticulitis, resection of the diseased bowel is indicated.2 5 In contrast, where the fistula has formed in the chronic setting, in the absence of a coexistent acute perforation or abscess formation, a conservative approach may be trialled. SVF can induce a localised inflammatory process rather than peritonitis and systemic upset.6 Therefore, the patient will likely have time to weigh up the risks and benefits of both conservative and surgical approaches.
In this case, optimisation of the patient’s Crohn’s medication regime was implemented. He was continued on infliximab. The patient expressed a preference for a conservative approach as he had already completed his family. There are a lack of publications discussing the conservative management of SVF in the setting of complicated Crohn’s disease; however, it has been a successful approach in the treatment of SVF resulting from other aetiologies.4 6–8
Sykora et al described a case of SVF in a 66-year-old man, which developed after undergoing a laparoscopic low anterior resection (LAP) for a large high-grade dysplastic polyp.8 This was treated conservatively by inserting a suprapubic catheter and starting antibiotic therapy. Although the total length of treatment was 4 months, on follow-up at 12 months, the patient was symptom free with no sign of fistula recurrence.8 In 2014, Kitazawa and colleagues also reported a case of SVF, 13 days after LAP for a rectal adenocarcinoma, in a 53-year-old man.6 This was treated conservatively using total parenteral nutrition and metronidazole for a 10-day period. Symptoms had fully resolved by discharge on postoperative day 41.6
There are limited data describing surgical approaches in the management of SVF. However, principles are deemed similar to that of surgical approaches to the seminal vesicle abscess, and fistulae in general.1 2 Fibrin glue deposition,9 transurethral drainage, transperineal drainage,10 percutaneous drainage and open surgery through a laparotomy5 have been described within the literature.
In 2014, Yumura et al ported a case similar to that herein.1 A 34-year-old man with complex Crohn’s disease was diagnosed with SVF. This patient also had symptomatic ischiorectal and perianal abscesses at the time of presentation. He did not respond to conservative treatments. He underwent colostomy formation. After 16 months, his abscesses and SVF had fully resolved. Furthermore, his semen count was low prior to surgery, but had returned to normal at the 16-month follow-up period. This approach may be indicated in younger men, who are yet to complete their family.
Patient’s perspective
I am happy to be involved in this case report, primarily to help doctors understand the range of problems faced by a chronic sufferer of Crohn’s. Also, with the probably vain hope that some significant development might help diminish the constraints the condition imposes on daily life for all sufferers.
In the early days of the condition, for the first nine years indeed—strictures where the dominant factor causing frequent bowel blockage and significant pain, distress, discomfort and almost complete debility, from time to time. This impacted greatly on daily life often resulting in many days in bed or hospital and therefore an inability to work or participate in any other activities. A bowel resection in 1994 significantly reduced subsequent blockage.
A combination of “range anxiety” and urgency are the primary restrictive factors of the condition. Country pursuits of which I would like to do more, are limited by lack of toilet availability. However with careful dietary restrictions—self learned—one can reduce urgency to a tolerable level.
I feel very involved in the management of my disease. I recently changed consultant, with whom a greater dialogue was possible and his empathetic approach, demeanour and preparedness to question and to listen carefully to the answers and to undertake thorough tests to ascertain exactly the condition of the bowel in order to prescribe the best course of treatment.
This too was described in considerable detail with the potential side effects of the recommended drugs also being brought to my attention and therefore the agreed decision of drug regime was reached through dialogue and some understanding.
In terms of delivery of care, the gastroenterology consultant asked many questions, listened carefully, understood and acknowledged the symptoms described bizarre though some of them may have seemed. Additional input was also sought from the surgical team, regarding the possibilities of rectifying the significant challenge posed by the bowel/bladder fistula.
A course of treatment was discussed in principle subject to various tests including CT and MRI scans, chest x-ray, ultrasound and numerous blood tests. Thereafter treatment was confirmed and is now well underway at the medical day unit where the nurses are most attentive empathetic and helpful.
In all honesty the care experience I have had is excellent in all ways. In the main, treatment of Crohn’s disease like most other conditions seems to be predicated on drug-based interventions. In my experience of managing this condition for over 30 years with only minimal daily drug use, the aspect which has had the greatest effect on day to day living is diet. Only by trial and error and our preparedness to methodically exclude certain foods from ones daily intake have I discovered how to calm the bowel by excluding major irritants.
The only suggestion therefore might be to engage a specialist dietician who might offer guidance to patients of potentially disruptive food, drink and alcohol thereby helping to calm the bowel on a day to day basis.
Crohn’s is a condition which need not be totally disruptive to the enjoyment of a full, happy and successful life. A clear understanding of the condition can be achieved by having a good relationship with your gastroenterologist from whom much can be learned. Thereafter read widely about your symptoms and the likely causes and be prepared to experiment with your diet to seek to establish which foodstuffs, drinks and alcohol most adversely affect you and be prepared to cut out the offending items which most irritate your bowl in order to give whatever drug regime you are prescribed the greatest chance of success, thereby minimising the adverse symptoms from which you suffer.
Learning points
Seminal vesicle fistulae (SVF) are a rare occurrence, irrespective of aetiology.
In the absence of acute pathology, conservative management may be trialled.
MRI allows for precise anatomical characterisation of SVF.
There is a paucity of literature specific to this pathology.
Case reports are required for our better understanding and implementation of appropriate management strategies.
Ethics statements
Patient consent for publication
Footnotes
Twitter @garifold
Contributors JT: Gained patient consent, performed literature review and discussion, and wrote the paper. AP: Reviewed imaging, provided images and wrote the investigations section of the paper. GN: Looked after the patient, had the case idea and performed corrections to manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.