Article Text

Summary
Stress cardiomyopathy is an acquired cardiomyopathy of unknown aetiology. It usually occurs in women over the age of 70 who have experienced physical or emotional stress. It is most commonly characterised by a transient, left ventricular systolic dysfunction in the apical portion and hyperkinesia in the basal segments, without obstructive coronary artery disease. Its association with obstructive hypertrophic cardiomyopathy and myocardial bridging is rare. Herein, we present such a case.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Stress cardiomyopathy occurring in a patient with an asymmetric septal hypertrophic cardiomyopathy and myocardial bridging of the left anterior descending coronary artery is rare. In our search, we found a similar case.
This case is fascinating in that it is difficult to comprehend having a severely hypertrophic heart, have the patient suffer a stressor and that very thick ventricle thins out completely and in a few days returns to being severely hypertrophic.
Case presentation
This is a black woman aged 67 years, with a known history of asymmetric septal hypertrophic cardiomyopathy, who 2 hours prior to admission developed atypical chest pain of mild to moderate intensity, with no other associated symptoms. The day prior, she had been under significant emotional stress due to financial issues at home. Her medications consisted only of metoprolol succinate 50 mg daily. She did not smoke, drink alcohol or use recreational/illicit drugs. Vital signs were normal and physical examination was remarkable for a 3/6 systolic ejection murmur heard at the left second intercostal space, and the presence of an S4.
Investigations
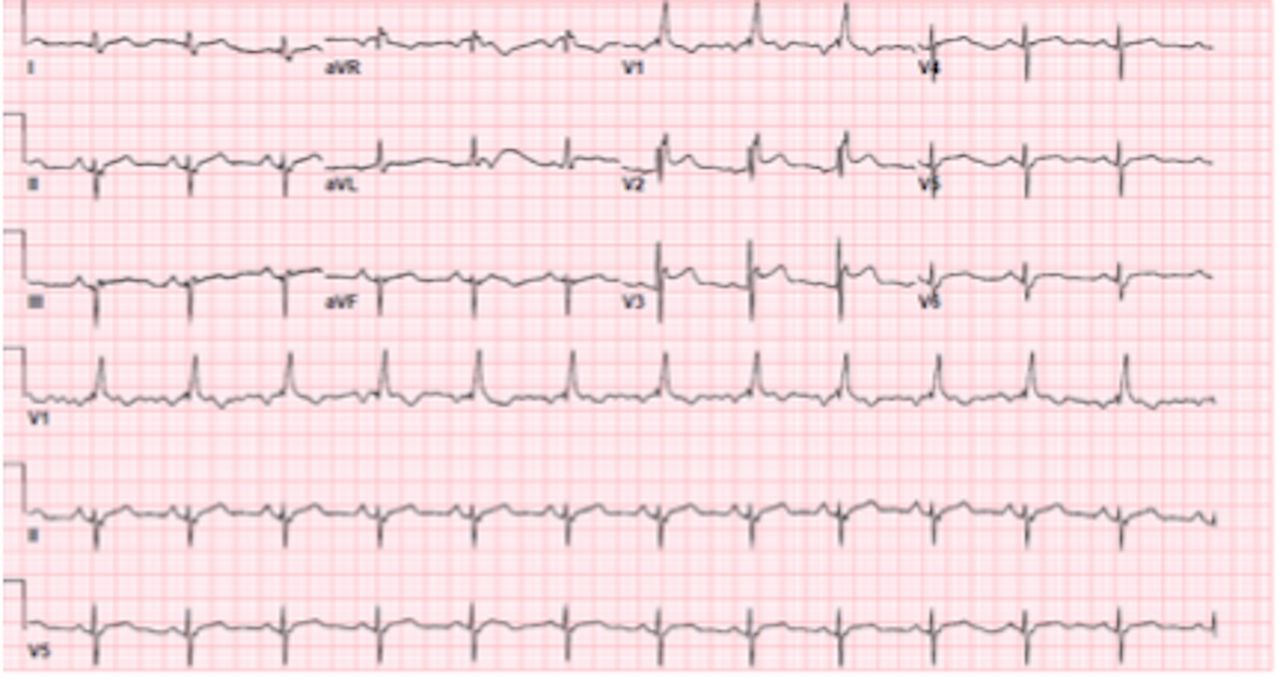
The laboratory studies were normal with the exception of Troponin I level being 1.7 ng/mL. An ECG performed demonstrated normal sinus rhythm with ST segment elevations in the precordial leads (figure 1). An echocardiogram performed demonstrated a reduced left ventricular ejection fraction of 35% with anteroseptal and apical akinesis, with systolic anterior motion of the mitral valve causing a left ventricular outflow tract gradient of 35 mm Hg (figures 2 and 3). Urgent coronary angiogram performed revealed normal coronary arteries with a dynamic systolic occlusion at the midportion of the left anterior descendant coronary artery consistent with myocardial bridging, and an ejection fraction of 35% with apical akinesis consistent with stress cardiomyopathy (figure 4).

ECG showing ST segment elevation in the precordial leads.
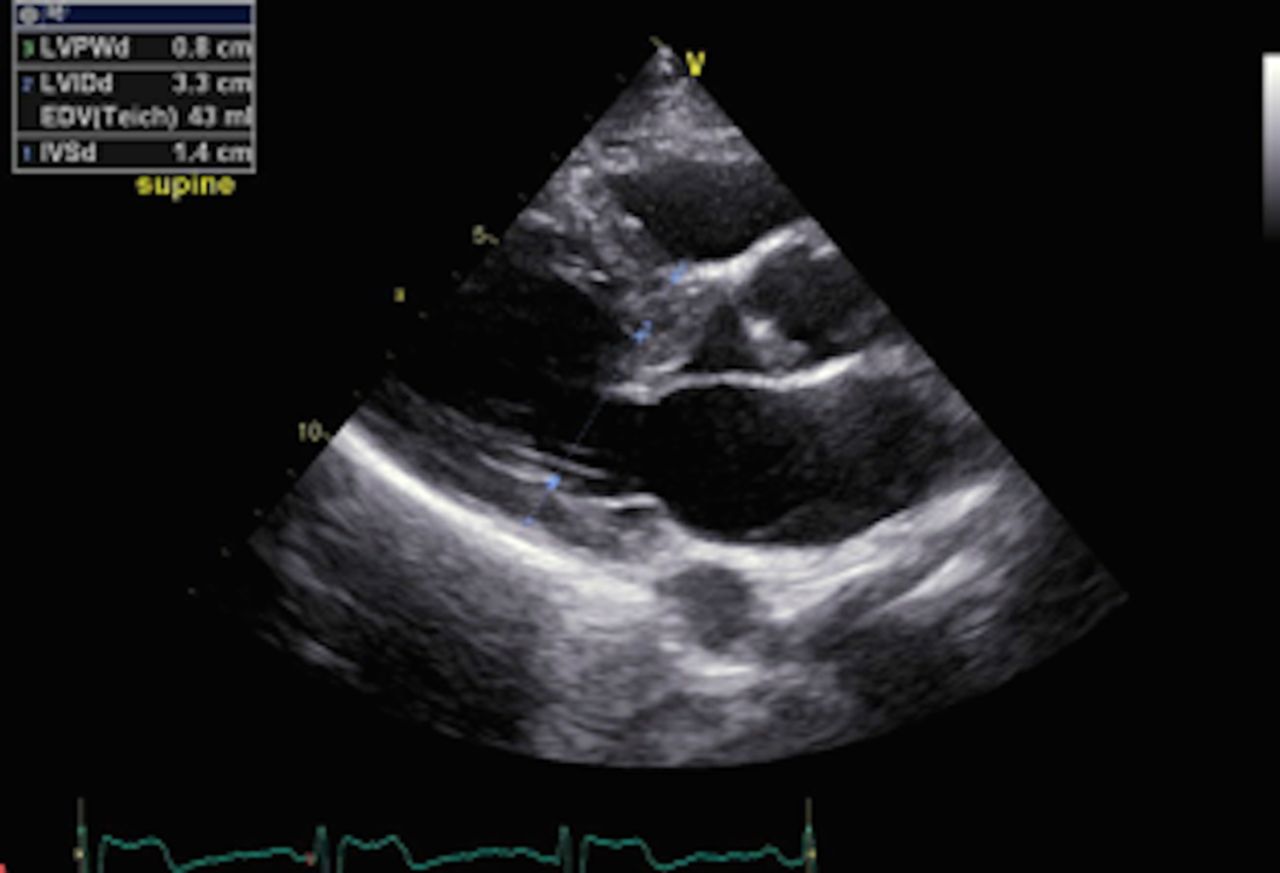
Transthoracic echocardiogram parasternal long-axis view demonstrating septal hypertrophy.

Transthoracic echocardiogram apical four-chamber view demonstrating apical ballooning, hypertrophic septum with systolic anterior motion of the mitral valve causing a left ventricular outflow tract gradient of 35 mm Hg.

Coronary angiogram and ventriculogram depicting a normal left anterior descending artery during diastole (A) and systole (B) depicting a narrowed segment of the midleft anterior descending artery, along with apical ballooning (C).
Outcome and follow-up
The patient did well throughout her hospital stay and was discharged on day 3 of her admission. Follow-up echocardiogram 2 weeks later demonstrated an ejection fraction of 65% and systolic anterior motion of the mitral valve with no change in the previously reported left ventricular outflow tract gradient (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transthoracic echocardiogram and ECG performed 2 weeks after discharge demonstrating an ejection fraction of 65%, a hypertrophic septum with systolic anterior motion of the mitral valve (left), along with resolution of the ECG changes (right).
Discussion
Stress cardiomyopathy is an acquired cardiomyopathy of unknown aetiology, but it most likely reflects the cardiac response to a surge of catecholamines.1 It affects ∼1–2% of all patients presenting with an initial diagnosis of an acute coronary syndrome or myocardial infarction. It is characterised by three distinctive features: (1) the presence of acute left ventricular wall dysfunction, (2) the absence of significant obstructive coronary artery disease and (3) the rapid improvement of left ventricular systolic function. The inhospital mortality with this entity is ∼1%, and complete recovery of the left ventricular dysfunction is seen in most patients by 4–8 weeks.1
The presence of myocardial bridging involving the midleft anterior descendant coronary artery has been shown to be associated with stress cardiomyopathy. In a study of 42 women with criteria of stress cardiomyopathy, myocardial bridging of the midleft anterior descendant coronary artery was noted on coronary angiogram in 17 cases (40%) and by CT angiography in 15 (with no myocardial bridging initially detected by coronary angiography).2 It was noted that, when compared with controls, there was a significantly higher incidence of myocardial bridging in patients with stress cardiomyopathy, p<0.007.
The presence of myocardial bridging in patients with hypertrophic cardiomyopathy occurs in approximately one-third of children, and in 15% of adults.3 The data on stress cardiomyopathy occurring in patients with hypertrophic cardiomyopathy are quite limited consisting mainly of isolated case reports.4 Moreover, the finding of stress cardiomyopathy in patients with hypertrophic cardiomyopathy and myocardial bridging is quite rare. A search of the literature yielded a case with similar findings as the case presented.4 This was a woman aged 54 years with quadriplegia, secondary to advanced motor neuron disease, who presented with chest pain and hypotension. Echocardiogram performed revealed apical ballooning of the left ventricle, septal thickness of 19 mm and systolic anterior motion of the mitral valve. Coronary artery angiography demonstrated a muscle bridge at the midleft anterior descending coronary artery and apical akinesis of the left ventricle. Another case of a patient with hypertrophic cardiomyopathy with midcavity obliteration, who developed a stress cardiomyopathy, demonstrated the development of left ventricular outflow tract obstruction. The authors concluded that in these cases, one may have a ‘moving left ventricular obstruction’.5
Learning points
Stress cardiomyopathy may occur in cases with hypertrophic cardiomyopathy.
Stress cardiomyopathy may develop in cases with myocardial bridging at the left anterior descending artery.
Do hypertrophic cardiomyopathy and/or myocardial bridging predispose to stress cardiomyopathy?
Footnotes
Contributors MB and JMVare responsible for conception and design, acquired and reported the data as well as analysed it. IA and OS are responsible for interpretation, reviewing and edition.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.