Article Text

Summary
Pituitary abscess is an uncommon pituitary lesion. Its clinical diagnosis can be difficult to distinguish from other pituitary lesions. This pathology is characterised by vague symptoms of headaches, generalised tiredness and hypopituitarism manifestations. A history of recent meningitis, paranasal sinusitis or head surgery can be a suggestive of the source of infection.
A 20-year-old man was admitted to neurosurgery department with complain of headache, fatigue, polyuria, polydipsia, blurred vision and sexual dysfunction. MRI of the head revealed a suprasellar mass that was centrally hyperintense lesion on T2-weighted images with peripheral hypointensity and isointense centrally on T1 images with peripheral hyperintensity images. Treatment of this lesion pituitary abscess was surgical drainage of the pituitary area through a trans-sphenoidal approach and broad spectrum antibiotic therapy with ceftriaxone, metronidazole and vancomycin for 6 weeks. The patient continues to have pituitary insufficiency and treated with oral hydrocortisone.
Although pituitary abscess is a rare condition, it should always be kept in mind when evaluating a patient with hypopituitarism. After the diagnosis, the surgery and antibiotics should be commenced rapidly. The outcome is usually good with proper treatment.
- Endocrine system
- Infections
- Pituitary disorders
- Infection (neurology)
- Neuroimaging
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
The pituitary gland is an endocrine gland about the size of a pea and weighs 0.5 gm in humans. Hormones secreted from the pituitary gland control: growth, blood pressure, certain functions of the sex organs, thyroid glands and metabolism as well as some aspects of pregnancy, childbirth, nursing, water/salt concentration and the kidneys, temperature regulation and pain relief.1 Different kind of lesions may develop in the pituitary gland which could lead to over or under secretion of hormone production and subsequently present as an incidental finding on imaging, symptoms of mass pressure or hormonal disturbances.
A rare pituitary lesion is a pituitary abscess. Pituitary abscess is very rare accounting for 0.2%–0.6% of all pituitary lesions. Only around 250 case reports have been described so far since the first case was described by Heslop in 1848.2 Pituitary abscess is an uncommon disease that usually presents with vague symptoms. To reach a diagnosis in such cases is usually difficult. The condition is considered a life-threatening one, however, fortunately the major number of cases have a rather chronic course. Based on different reports, theses abscesses are characterised by the following: it constitutes less than 1% of all the pituitary diseases being seen by the specialist; higher female predominance; the age range is between 12 to 76 years and the average period between onset the symptoms and diagnosis is 8 months.3
Preoperative diagnosis is a dilemma as symptoms such as pituitary abnormal function are non-specific, radiological findings are not distinctive of an abscess and symptoms like headache or visual disturbances are vague. In addition, infectious symptoms such as fever, meningism and high white cell count (WBC) are not seen in around 70–8% of cases. Therefore, majority of the cases are diagnosed either post mortem or postoperatively.4
Pituitary abscess can develop in a normal pituitary gland (about 70%) or in pre-existing pituitary pathology (about 30%). Of the pre-existing lesions, a pituitary adenoma is most common, followed by a Rathke’s cleft cyst, craniopharyngioma and lymphoma.5 The therapies available are trans-sphenoidal surgery, antibiotics and hormonal replacement.
Case presentation
A 20-year-old Bahraini man presented to accident and emergency department in Salmaniya Medical Complex (Manama/Bahrain) in Mach 2016 complaining of headache which he described as severe, continuous and exacerbated with exposure to bright light. In addition, he complained of photosensitivity, nausea, left eye blurred vision and generalised body fatigue. These symptoms were worsening over a month period of time. He denied history of limb weakness, abnormal movements or seizure, loss of consciousness or sensory manifestations.
He was initially managed with analgesia and in view of his alarming symptoms MRI brain was requested.
Investigations
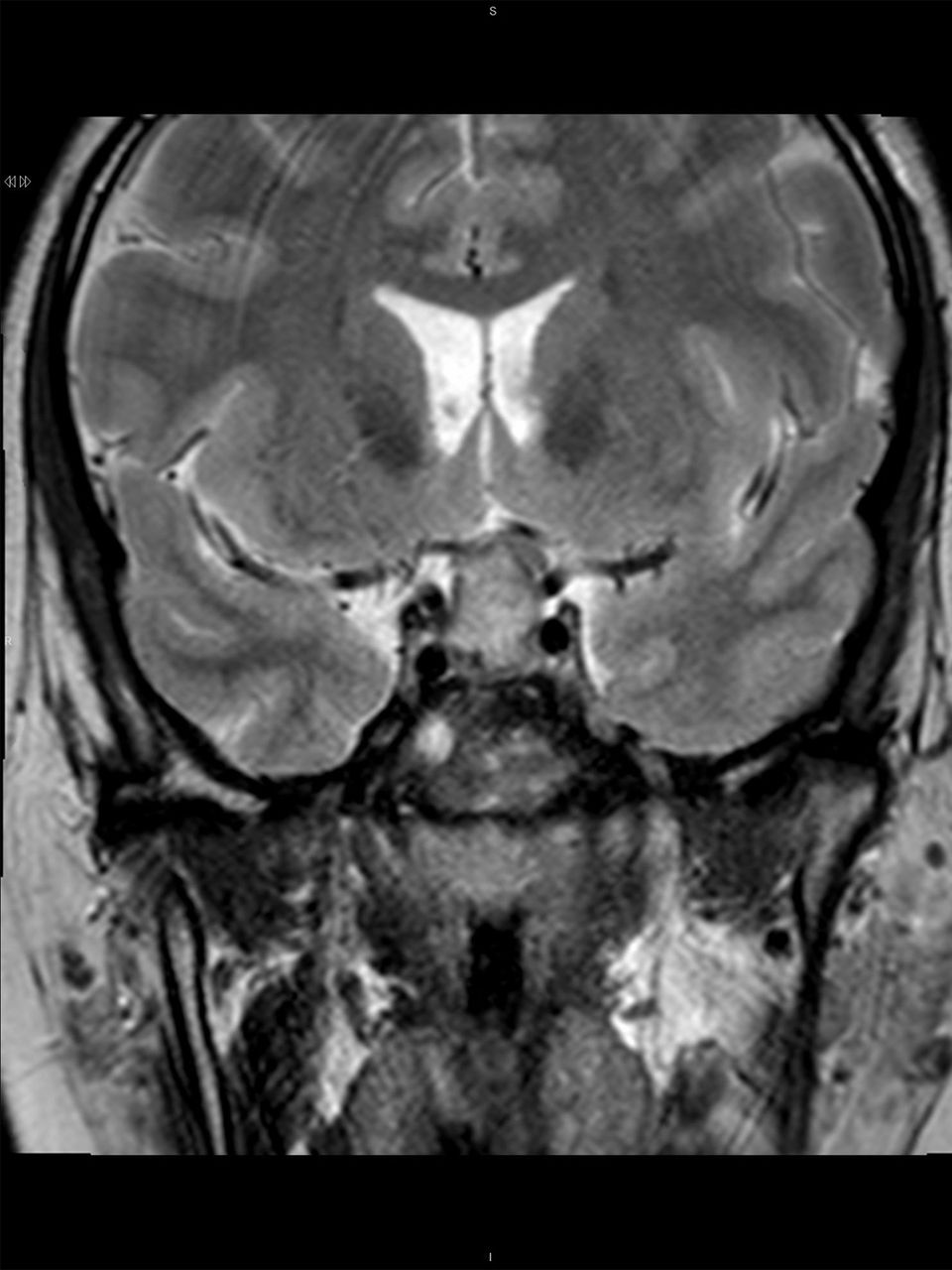
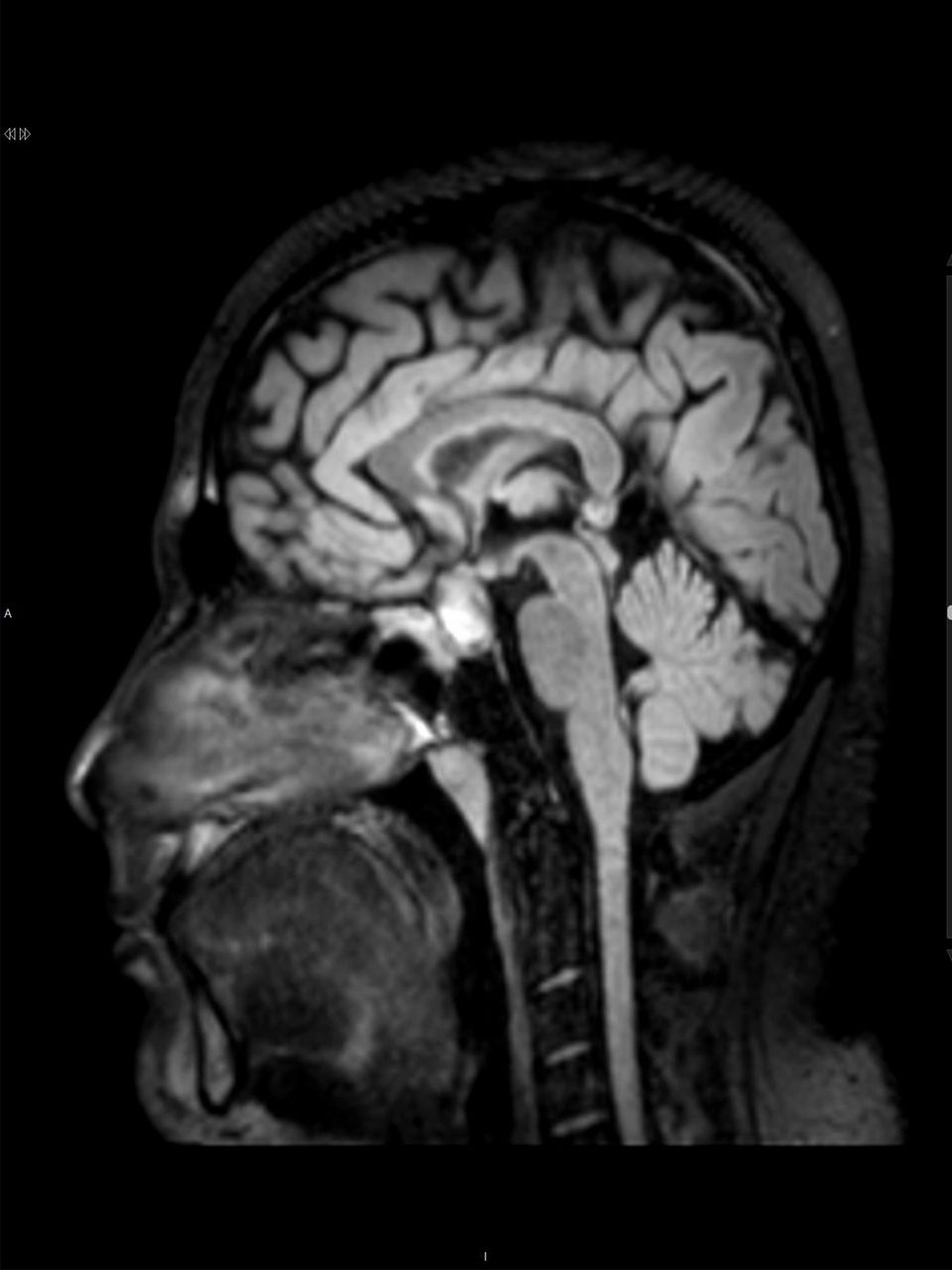
Multiplanar multisequential images were taken with postimage, and preimage contrast was given. The scan showed presence of heterogeneously hyperintense lesion on T2-weighted images with peripheral hypointensity (figure 1 and not suppressed on fluid-attenuated inversion recovery images (figure 2). The optic chiasm was compressed and displaced superiorly by the lesion. Both cavernous sinuses were mildly compressed too with sparing of internal carotid artery blood flow. T1 images with no contrast showed fluid level (figure 3).
MRI fluid-attenuated inversion recovery image (sagittal view) the sphenoid sinus filled with debris and thick mucosal lining.

MRI T2 image (frontal view) sellar/suprasellar mass that was isohyperintense with peripheral hyperintensity

{kind=link}
{kind=link}
{kind=link}
MRI T1 image (sagittal view) non-contrast fat saturated showing fluid level
Therefore, the conclusion was suggestive of macroadenoma of pituitary gland (size 1.8×1.5×1.3 cm in size) with haemorrhage and a mass effect on optic chiasm.
In view of the MRI findings, pituitary hormonal assessment was done. Furthermore, the patient gave history of loss of libido, failure of erection, polyuria and polydipsia but denied any gynaecomastia or change in body part size. The results showed central hypogonadism, central hypoadrenalism, normal thyroid function and mildly elevated level of prolactin. He was commenced on hydrocortisone oral tablet (20 mg on morning, 10 mg on evening doses). On examination, patient did not show any cranial nerve, limb or gait abnormalities. There was no thyromegaly or signs of acromegaly. A chest X-ray done was normal (table 1).
Patient’s laboratory results and normal ranges
Differential diagnosis
Pituitary adenoma
Pituitary abscess
Pituitary haemorrhage
Treatment
After investigating the patient, he was scheduled for theatre by July 2016 for trans-sphenoidal removal of the pituitary macroadenoma. Intraoperatively the patient was kept on left side 20° with an incision done in the right nostril, the mucosa was separated and the sphenoid sinus mucosa removed. The sellar floor identified and removed. Thick capsule of abscess incised with yellowish pus was drained. The cavity was cleaned and irrigated with antibiotics and saline. The pus was sent for Gram stain, culture, acid-fast bacilli (AFB) stain and histopathological evaluation. The pituitary was not removed.
The histopathology showed features suggestive of inflammatory lesion possibly an abscess. There is no evidence of pituitary adenoma in this small and partly compressed biopsy. The Gram stain showed few WBC and a sterile culture. AFB stain did not show any acid fast bacilli.
Outcome and follow-up
Postoperatively, the patient was shifted to intensive care unit for overnight observation. After that, he was transferred to a neurosurgery ward. He was commenced on the following antibiotics: metronidazole 400 mg three times per day, ceftriaxone 1 g once per day and vancomycin 1 g two times daily for a total of 6 weeks. He was doing well with improvement in symptoms and normal functional status.
The patient continued to have pituitary insufficiency on follow-up and the hydrocortisone as continued. No further headaches have been noticed or other symptoms. Follow-up MRI was done and showed no more enhancing residual abscess pockets within the pituitary fossa suggesting complete resolution.
Discussion
Pituitary abscesses are divided into two types: primary and secondary. The primary subtype constitutes the majority of the pituitary abscess cases. On the other hand, the secondary subtype usually rises from within an existing pituitary lesion. It can be caused by a haematogenous or direct spread from distant lesions such as meningitis or sinusitis. Vates et al reviewed 24 cases of pituitary abscess. The study showed that 19.7% of the affected patients had a positive history of sepsis or an obvious source of bacteraemia, 12.5% gave history of cerebrospinal fluid (CSF) leak in the sense of rhinorrhoea, 41.7% had history of pituitary surgery or sphenoid sinus disease, 8.3% with history of brain radiation and 4.2% had a chronic history of sphenoid inflammation and disease.6 On the other hand, another study by Lindholm et al did not show an infectious cause in 9 out of 21 cases of pituitary abscess. Furthermore, Jimeno et al described that most likely the primary source of the pituitary abscess was from the spread of infection from a maxillary or frontal sinusitis.7 8 In other reports, cavernous sinus thrombosis was once suggested that it may play a role in pituitary infection and inflammation.9 In our case, there was a strong suspicion that source of infection was due to direct spread from the sphenoid sinuses as the MRI showed evidence of chronic inflammation and mucosal thickening despite that the patient denied any symptoms of upper respiratory or sinusitis.
The organisms mostly isolated from pituitary abscesses are Gram-positive cocci (mainly Staphylococcus and Streptococcus), Gram-negative organisms such as Neisseria, Escherichia coli and Corynebacterium. Others less likely to be isolated organisms are fungi and parasites.10 However, the majority of the pituitary abscess cultures have been reported to be sterile. The reason for this could be because of the use of antibiotics preoperatively or the laboratory techniques used was inappropriate for the growth of fungus or anaerobic organism.11 It was suggested once that pituitary abscess does not represent a bacterial infection. It is just an inflammatory reaction secondary to pituitary infarction. As the high frequency of the sterile cultures and along with it, the associated endocrine abnormalities can be explained by simple inflammation of the gland.12
Radiologically, it still very challenging to differentiate between a pituitary abscess and adenoma. The CT and MRI (including the diffusion-weighted images) findings of both conditions are more or the less the same for both conditions. Shimamura et al suggests that a way of differentiating both pituitary lesions is by the high uptake of the abscess on thallium-210 single-photon emission CT on the early and delayed images.13
Surgical drainage is the standard treatment for a pituitary abscess. The trans-sphenoidal approach is the recommended approach; however, craniotomy is preferred if the abscess is suprasellar or significant evacuation is considered difficult. The operation is considered invasive and traumatic procedure. Complications of surgery include meningitis, vascular injury and CSF leakage. The incidence of complications is decreasing with the development in medical practices.14
The operation could also increase the risk of or delay the recovery from anterior pituitary insufficiency and diabetes insipidus. Liu et al reported that only 8 of the 30 patients (including 3 patients who had normal preoperative pituitary function) attained normal pituitary function following surgery. The rest of the patients continued to require hormone replacement therapy, and 6 of the 21 patients with preoperative diabetes insipidus required postoperative desmopressin acetate.15 Therefore, the surgery can also lead to destruction of the pituitary gland.14 Broad-spectrum antibiotic therapy must be started as soon as the diagnosis of pituitary abscess is confirmed. After identification of the organism, a specific antibiotic therapy should be continued for 4 to 8 weeks.
Although pituitary abscess is a rare condition, it should always be kept in mind when evaluating a patient with hypopituitarism. This case presents on of the rare causes of pituitary insufficiency. A pituitary abscess must be tickled in the differential diagnosis of a patient with hypopituitarism and signs of systemic infection, and the patient should have an MRI assessment. Treatment consists of debridement, systemic administration of antibiotics and hormonal replacement.
Learning points
Pituitary abscess should be kept in mind in the differential diagnosis of a pituitary mass.
Surgical intervention is the treatment of choice followed by prolonged course ofintravenous antibiotics.
The pituitary should have follow-up with brain MRI and to rule out hormonal deficiencies with appropriate hormonal replacement.
References
Footnotes
Contributors JMAS managed the patient from infectious perspective and supervised the writing of the case report. RAMBAA managed the patient from infectious perspective and wrote the case report. MH managed the patient for the neurosurgery perspective.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Hospital Ethical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.