Article Text

Statistics from Altmetric.com
Description
A woman in her mid-80s presented with sudden onset severe chest pain radiating to her left shoulder. A 12-lead ECG showed anterolateral ST-segment elevation with loss of R waves, consistent with an acute myocardial infarction (figure 1A).

(A) ECG on admission showing anterolateral ST-segment elevation with loss of R waves, consistent with an acute myocardial infarction. (B) ECG on follow-up at 3 months showing evidence of recovery of anterior R waves on ECG.
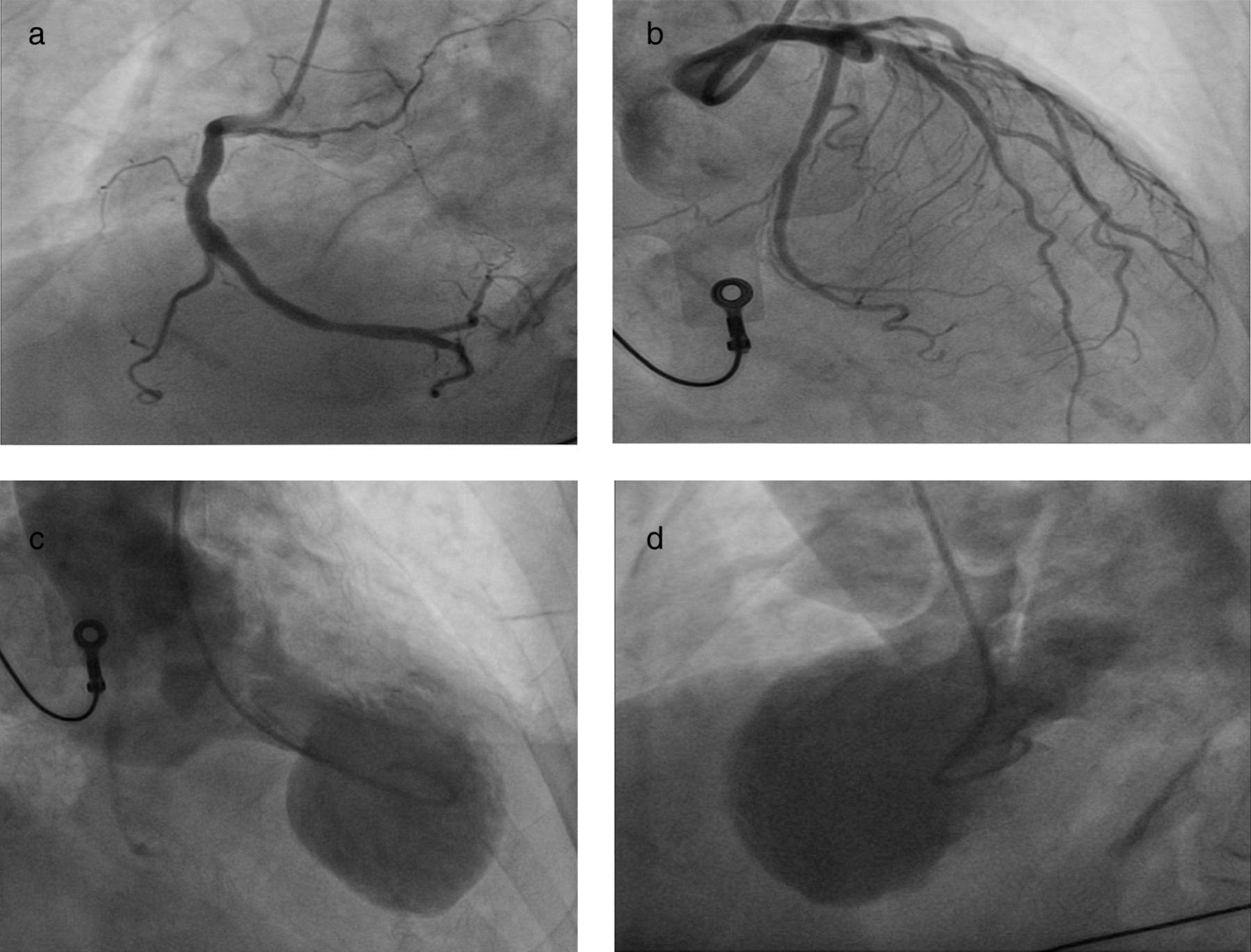
Emergency coronary angiography revealed unobstructed coronary arteries with only mild atheroma (figure 2A,B). Left ventriculography confirmed anteroapical ballooning of the left ventricle (figure 2C,D) consistent with takotsubo cardiomyopathy. Although no proximate emotional insult was evident she had recently dealt with the bereavement of a close family member.

(A and B) Coronary angiography confirming unobstructed coronary arteries. (C and D) Left ventriculography revealed anteroapical ballooning of the left ventricle ,consistent with takotsubo cardiomyopathy.
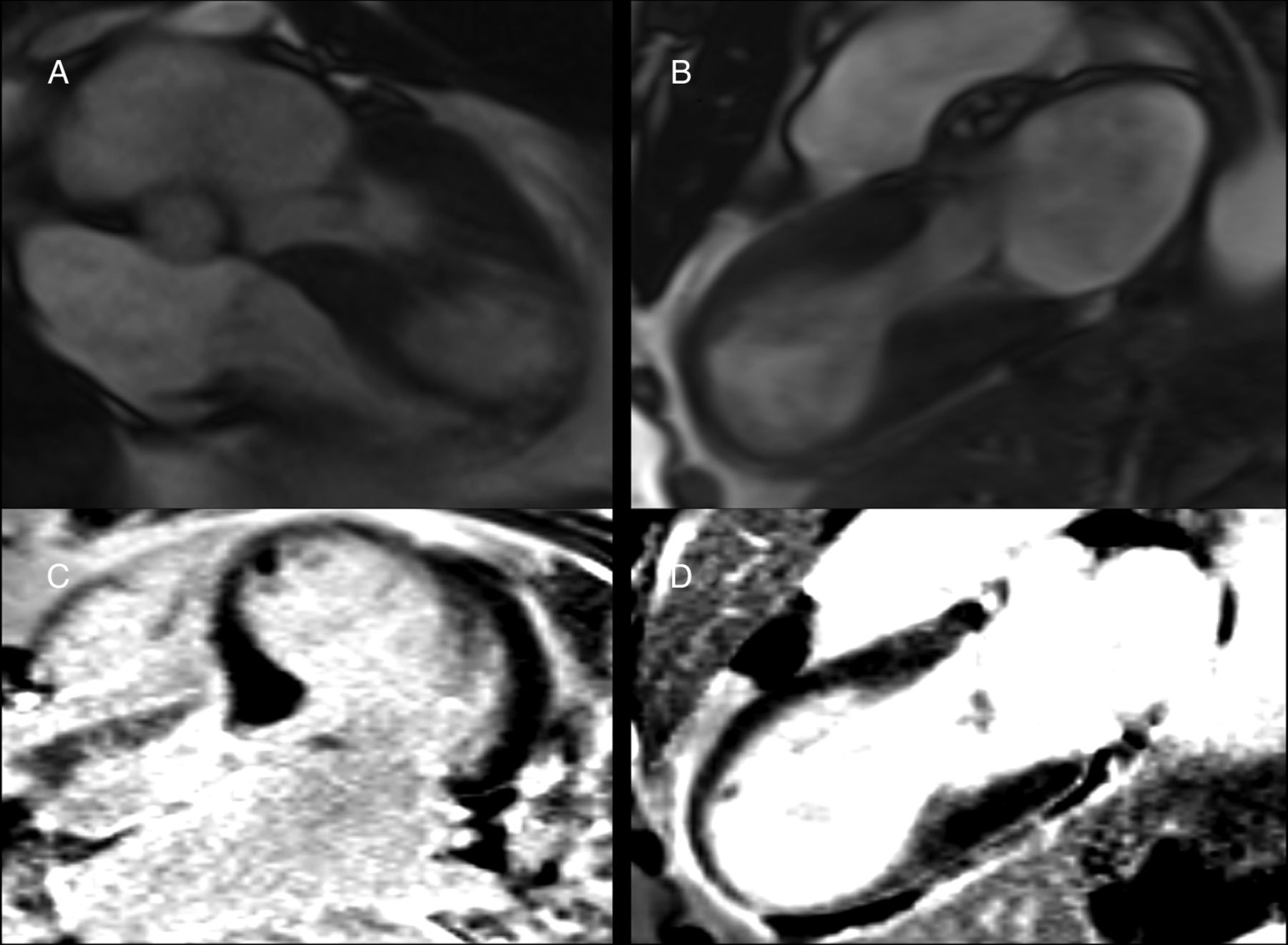
A transthoracic echocardiogram in the coronary care unit confirmed moderately impaired left ventricular (LV) function (ejection fraction 40–45%). High-sensitive troponin-T peaked at 195 ng/L (normal <14 ng/L). Cardiac MRI revealed thinned and akinetic apical segments of the LV (figure 3A,B) making it difficult to differentiate scarred myocardium (eg, due to old myocardial infarction) from stunned myocardium secondary to takotsubo cardiomyopathy. There was no late myocardial gadolinium enhancement (figure 3C,D).
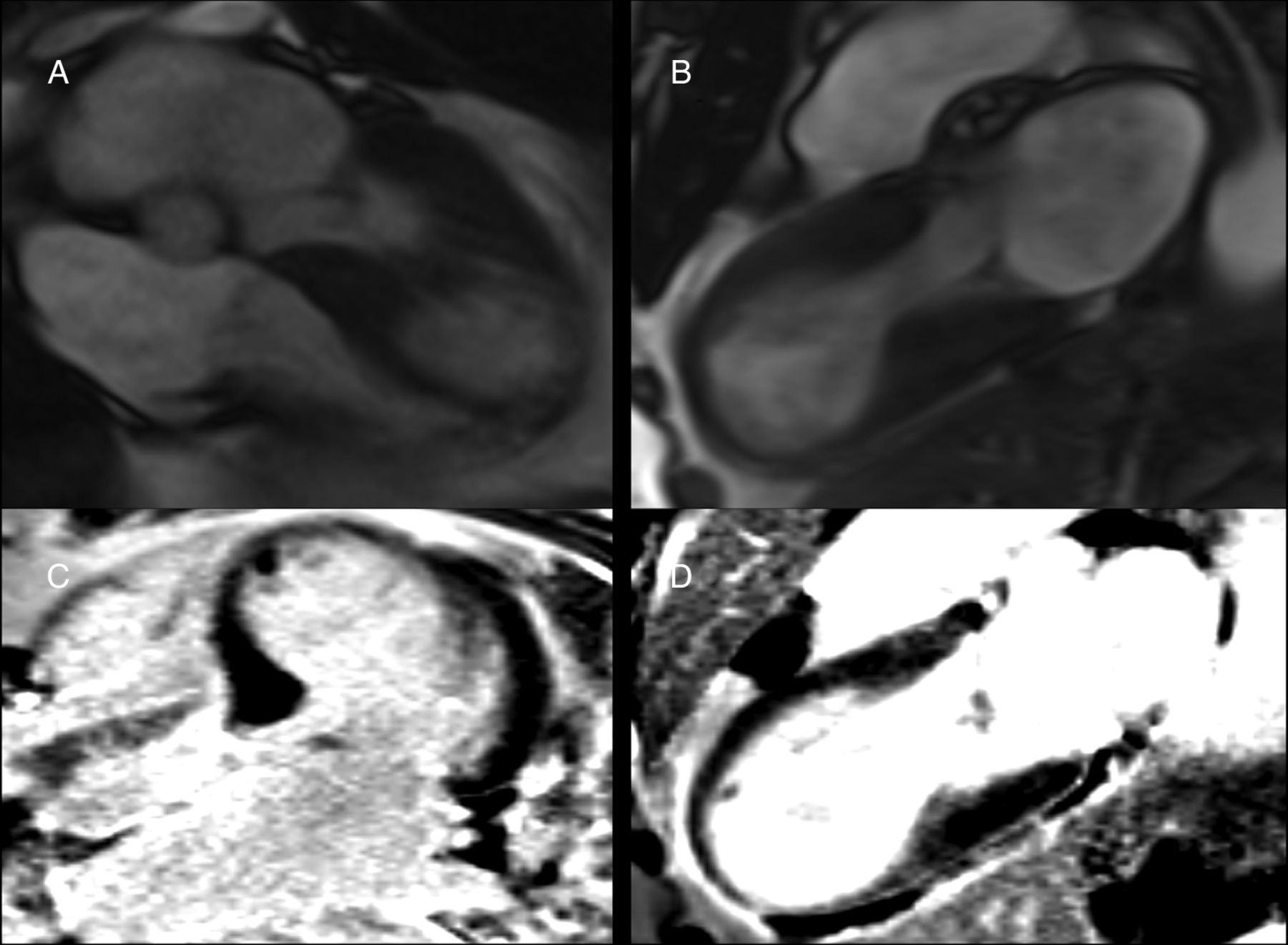
(A and B) Thinned and akinetic apical segments of the left ventricular. (C and D) There was no late myocardial gadolinium enhancement.
The patient made a complete functional recovery and was discharged home on no medication. On follow-up at 3 months, the patient was asymptomatic with evidence of recovery of anterior R waves on ECG (figure 1B). There was complete resolution of the apical wall thinning and akinesia demonstrated on repeat cardiac MRI at 3 months (figure 4A,B) with no late myocardial gadolinium enhancement (figure 4C,D).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A and B) Complete resolution of the apical wall thinning and akinesia. (C and D) No late myocardial gadolinium enhancement at 3 months.
Learning points
-
Takotsubo cardiomyopathy (TCM) or apical ballooning syndrome is a well-recognised clinical entity. Although the pathophysiological mechanisms are not fully understood the apical ballooning that results is thought to occur due to a sudden catecholamine surge1 and acute stress has been indicated as a precipitant for the transient left ventricular apical ballooning in about a quarter of cases.2
-
Comparative studies in patients with acute myocardial infarction or TCM have found cardiac MRI scanning to be a useful tool in the acute setting. Subendocardial hypoenhancement is not seen in patients with TCM as was the case in our patient.3
-
The patient had dramatic myocardial thinning evident on cardiac MRI with loss of R waves on her ECG making it difficult to differentiate her presentation from a previous myocardial infarction.
Footnotes
-
Contributors AB was involved in the acquisition of data and analysis and drafting of the article. NN was involved in the drafting of the article. RS was involved in the acquisition of data and analysis. SQK was involved in the conception and design, revision of the article and final approval.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.