Article Text

Statistics from Altmetric.com
Description
A 60-year-old man presented with sudden onset of ptosis of the right eye. There was no history of headache, fever, altered sensorium, vision loss, trauma, diabetes or weakness of the limbs. On examination, there was right-sided third nerve palsy (figure 1). The rest of the neurological and systemic examination was normal. The patient's brain MRI was normal apart from pagetoid bony changes as evidenced by large well-defined lytic and sclerotic lesions in the skull along with diploic widening.

Face of the patient showing ptosis of the right eye.
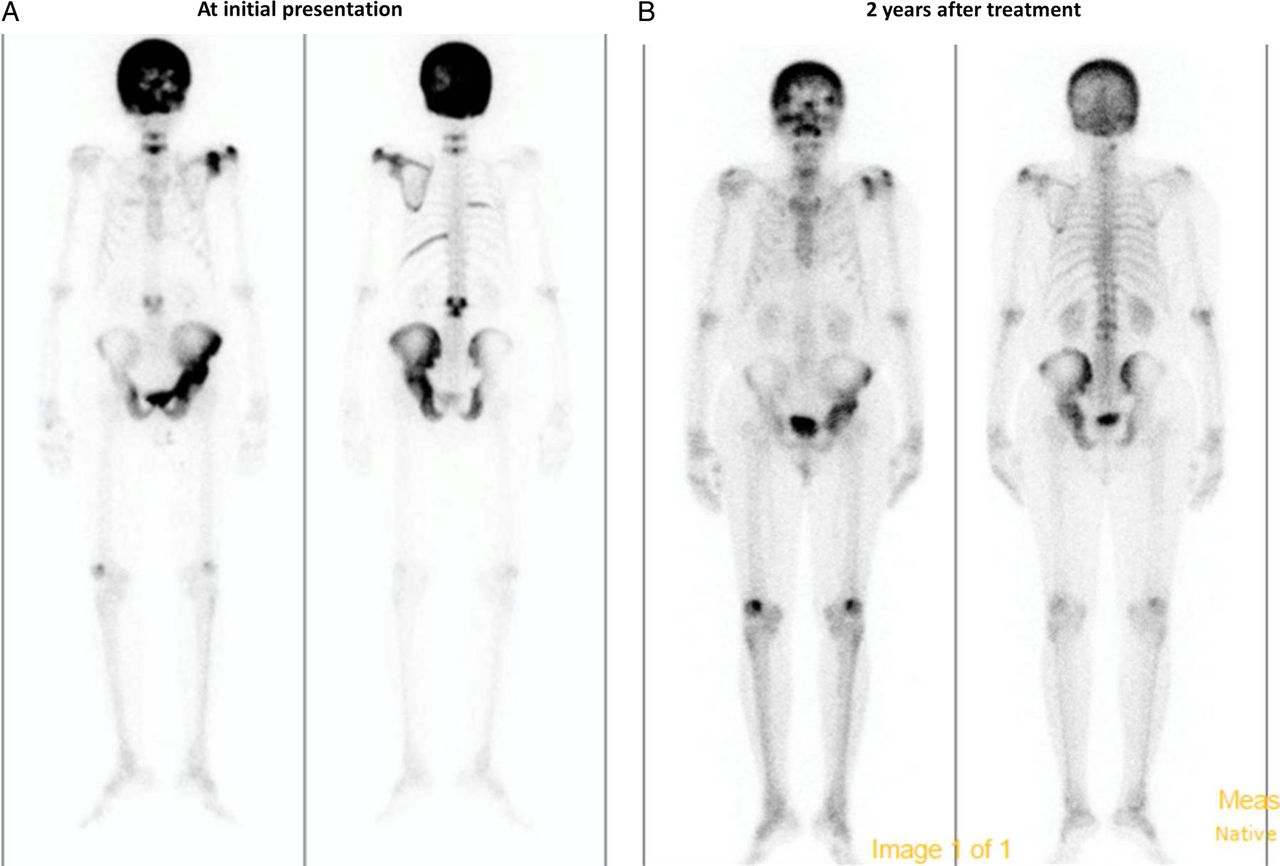
Blood investigations were normal except for markedly elevated alkaline phosphatase of 2171 μ/L (normal 40–125). The patient's skull X-ray revealed both osteolysis and osteosclerosis. His technetium bone scan showed marked uptake in the skull and left hip suggestive of polyostotic Paget's disease of bone (PDB; figure 2A). He was treated with yearly zoledronic acid. He had complete resolution of his neurological deficit within 2 months with a significant decline in the alkaline phosphatase (1567 μ/L). At 2-year follow-up, his alkaline phosphatase was normal (84 μ/L) and bone scan showed a marked regression of the disease (figure 2B).
{kind=link}
{kind=link}
(A) Technetium bone scan showing marked uptake in the skull and left pelvis. (B) Follow-up technetium scan (after 2 years) displaying regression of the uptake.
PDB is a disease of osteoclasts where there are areas of marked bone resorption followed by abnormal new bone formation. It usually presents after the age of 55 years and the highest prevalence has been reported from the UK. The SQSTM1 (sequestosome-1 encoder) gene has been shown to be associated with this disease.1 Bone pain, deformities, fractures and neurological complications such as headache, hearing loss and nerve palsies have been reported as the manifestations of PDB. The skull and pelvis are usually involved.2 Third nerve palsy is a rare presentation of this disease and is due to the compression of the nerve as it enters the superior orbital fissure.3 Diagnosis is usually established by finding marked elevation of alkaline phosphatase, bone scan showing marked uptake in the affected bones and X-ray showing both osteosclerosis and osteolysis. Treatment of this disease includes establishing adequate calcium and vitamin D nutrition and using antiresorptive agents such as zoledronic acid.1
Learning points
Bone pains, deformities, fractures and neurological complications such as headache, hearing loss and nerve compression syndromes resulting in nerve palsies may be the initial presentation of Paget's disease of bone.
Management of this condition usually involves maintaining adequate calcium and vitamin D nutrition and using antiresorptive agents such as zoledronic acid.
Acknowledgments
The authors thank Ms Banu Shankar for secretarial help.
Footnotes
Contributors SS and NK wrote the manuscript. JH and TVP reviewed the manuscript. SS, NK, JH and TVP approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.