Article Text

Abstract
The course and distribution of the facial corticobulbar tract (CBT) was examined by correlating MRI of brain stem lesions with neurological symptoms and signs including central (C-FP) or peripheral facial paresis (P-FP) in 70 patients with localised infarction of the lower brain stem. C-FP occurred more often in patients with lesions of the lower pons or upper medulla of the ventromedial brain stem. Some patients with dorsolateral infarcts of the upper medulla to the lower pons showed C-FP, mostly on the lesion side. P-FP on the side of the lesion was also seen in patients with dorsolateral involvement of the lower pons. Patients with ventromedial infarction of the brain stem showed paresis of extremities contralateral to the lesion. Specific neurological symptoms and signs such as dysphagia, vertigo, nystagmus, Horner's syndrome, ipsilateral cerebellar ataxia, and contralateral superficial sensory impairment were seen in patients with dorsolateral infarcts of the brain stem. It is hypothesised that the facial CBT descends at the ventromedial lower pons, near the corticospinal tract, mainly to the level of the upper medulla, where the fibres then decussate and ascend in the dorsolateral medulla to synapse in the contralateral facial nucleus.
- facial nerve
- corticobulbar tract
- brain stem
- magnetic resonance imaging
Statistics from Altmetric.com
The facial nucleus in humans is located dorsolaterally in the caudal pons.1 2 The corticobulbar tract fibres (CBT) that connect the motor cortex with the facial nucleus provide strongly unilateral innervation to the contralateral lower facial muscles and bilateral innervation to the upper facial muscles.1-4Classic symptom localisation has postulated that lesions rostral to the upper mid-pons result in contralateral facial paresis of central type (C-FP), whereas ipsilateral facial paresis of peripheral type (P-FP) ensues from lesions involving the inferolateral part of the pons.1 5 We previously reported on two patients in whom contralateral C-FP resulted from ventromedial medullary infarction, concluding that the facial CBT consists of looping fibres that descend at least to the medullary level and then decussate.6 The present study describes our further attempt to clarify the course and distribution of the facial CBT in a larger group of patients with lower brain stem infarction.
Patients and methods
The present study investigated 70 patients admitted to our department at Aichi Medical University Hospital with acute infarction of the caudal portion of the brain stem between 1989 and 1998. The patients comprised 51 men and 19 women with an age range of 38 to 86 years. Brain MRI was performed within 2 weeks of symptom onset in all patients. For MRI, T1 and T2 weighted images were obtained in both the axial and coronal planes. In the present study, all patients had symptomatic and localised infarctions in the lower brain stem. These were not present in patients with fatal extensive lesion or multiple lesions of the infarct. Patients were classified into the following six groups according to the location and distribution of ischaemic lesions as detected by MRI. Group A (ventromedial involvement at the lower pontine level) comprised seven men and four women with an age range of 58 to 73 years; the lesion was on the right side in six and the left in five. Group B (ventromedial involvement at the upper medullary level) comprised five men and one woman with an age range of 40 to 70; the lesion was on the right in three and the left in three. Group C (ventromedial involvement of the middle to lower medulla) comprised two men and one woman with an age range of 53 to 60; the lesion was right in one and left in two. Group D (dorsolateral involvement of the middle to lower medulla) comprised eight men with an age range of 40 to 83; the lesion was right in four and left in four. Group E (dorsolateral involvement of the upper medulla) comprised 20 men and six women with an age range of 38 to 84; the lesion was right in 14 and left in 12. Group F (dorsolateral involvement of the lower pons) comprised nine men and seven women with an age range of 40 to 86; the lesion was right in seven and left in nine Attempts were made to determine the rostral and caudal levels of the crossing of facial CBT fibres and to localise the descending and ascending fibres from frequencies of occurrence of C-FP or P-FP and other brain stem signs. Furthermore, to elucidate the course and location of facial CBT in axial sections of the brain stem, a comparative analysis was conducted of major neurological symptoms and signs among the six groups.
Results
FREQUENCY OF OCCURRENCE OF C-FP AND P-FP (TABLE1)
A C-FP occurred in 29 of the total 70 patients. The C-FP seen in these patients was relatively mild, and recovery was almost complete within 1 to 2 months of onset. All 11 patients of group A (ventromedial involvement of lower pons) showed C-FP on the side opposite to the lesion. Among the six patients of group B (ventromedial involvement of upper medulla), four patients (67%) showed C-FP on the side opposite to the lesion. The remaining two patients (33%) showed no evidence of C-FP. In group C (ventromedial involvement at the middle to lower medulla), C-FP was not present in any of the three patients.
Facial paresis in patients with lower brain stem infarcts
Of the eight patients in group D (dorsolateral involvement of the middle to lower medulla), only one (13%) developed C-FP on the side of the lesion. A C-FP was also clinically present in 10 of the 26 patients in group E (dorsolateral involvement of the upper medulla), and C-FP of the nine patients (35%) was on the side of the lesion and one patient (4%) on the opposite side. Of the 16 patients in group F (dorsolateral involvement of the lower pons), P-FP occurred on the side of the lesion in 11 patients (69%), and C-FP in another three (19%).
FREQUENCY OF MAJOR SYMPTOMS AND SIGNS IN PATIENTS WITH LOWER BRAIN STEM INFARCTS (TABLE 2)
In the three groups with ventromedial involvement of the lower brain stem (A, B, C), hemiplegia on the side opposite to the lesion was a common sign. None of the patients in these three groups showed symptoms or signs which were seen the patients with involvement of the dorsolateral part at the level of lower brain stem. Two patients (18%) of group A and two (33%) of group B had deep sensory impairment of the limbs and trunk on the opposite side.
Frequency of major symptoms and signs in patients with lower brain stem infarcts
In the remaining three groups with dorsolateral involvement of the lower brain stem (D, E, F), contralateral limb paresis occurred in only three patients (12%) belonging to group E. In patients with these dorsolateral infarcts, a wide variety of symptoms and signs of involvement such as dysphagia, vertigo, hiccups, hoarseness, nystagmus, paralysis of the soft palate, Horner's syndrome, facial sensory impairment, ipsilateral cerebellar ataxia, and contralateral superficial sensory impairment of limb and trunk were present.
Discussion
Some CBT fibres in humans are thought to leave the corticospinal tract (CST) in the brain stem,7-11 with a portion of them descending in the medial lemniscus as an aberrant pyramidal tract, although their precise topographic anatomy is not clear.3 7 10 To explain C-FP from lesions caudal to the facial nucleus, damage to the aberrant pyramidal tract has been postulated, including involvement of the classic Pick's bundle,12-15 which reverses course in the pyramidal decussation and ascends in the CST to connect with the motor nuclei of some cranial nerves. However, whether or not the facial nucleus actually receives such CBT fibres has not been determined.3 16 17
Currier18 has hypothesised that facial CBT fibres leave the pyramidal tract at the pontomedullary junction and descend caudally to at least the middle medullary levels before most of them cross to the opposite facial nucleus. Interruption of these fibres by infarction at a predecussation level has been postulated to result in a contralateral C-FP. Cavazos et al 19 have described some fibres of the facial CBT as descending ipsilaterally, making a loop as caudally as the upper medulla before decussating and ascending to the contralateral facial nucleus. Our results indicate that C-FP occurred more often in patients with a lesion extending from the lower pons to the upper medulla than in those with a lesion in the middle to lower medulla, regardless of whether the lesion was located ventromedially or dorsolaterally. Kimet al 20 have also reported that, in patients with lateral medullary infarction, C-FP was seen more often with high than middle to low medullary lesions.
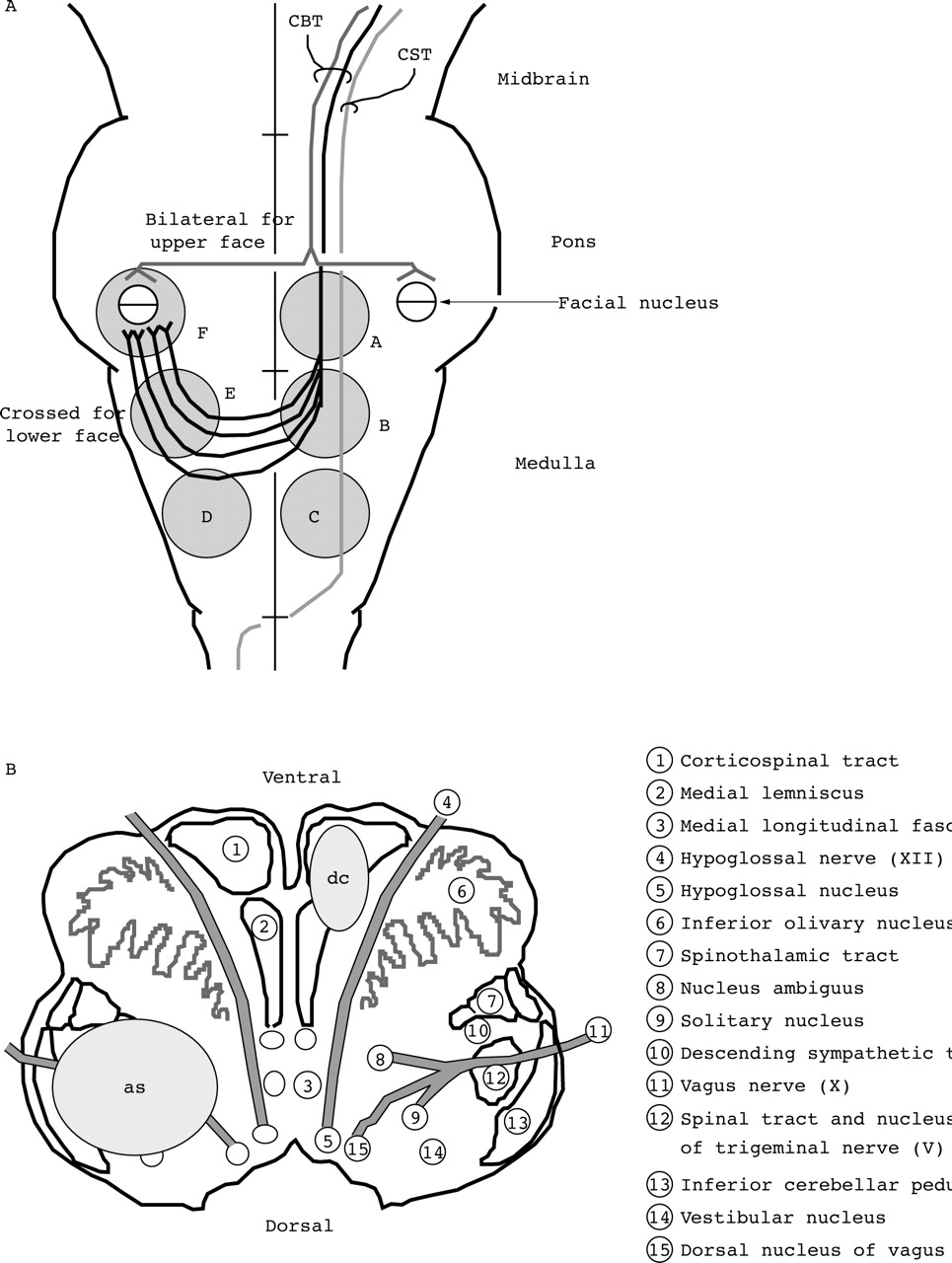
Our present findings suggest that the facial CBT descends at least to the level of the upper medulla, where the fibres cross the midline, even though their specific topographic anatomy may vary from one person to another (figure A). The facial CBT, then, could be represented as looping fibres, most of which decussate in the upper medulla. This schema is an alternative to placing these CBT fibres in the aberrant pyramidal tract, which reverses course in the lower medulla to ascend from the pyramidal decussation. Jennyet al 4 have reported that descending CBT fibres innervated the lower facial motor nuclear region bilaterally in the monkey, although with contralateral predominance. Therefore, non-decussating CBT fibres supplying the ipsilateral lower facial nucleus may be present in humans.4 21 On the basis of locations of facial CBT seen in axial sections, we would argue that these CBT fibres descend near the CST, mostly to the upper medulla, where they decussate and ascend in the dorsolateral medulla to connect with the facial nucleus (figure A and B). On the other hand, as C-FP resulting from involvement of ascending pathways occurred less often than C-FP from involvement of descending pathways; these ascending pathways may be widely dispersed in the dorsolateral medulla rather than representing a discrete bundle.

{kind=link}
(A) Schematic diagram of pathways of the facial corticobulbar tract (CBT). The corticospinal tract is designated CST. The six grey areas show the locations of lower brain stem infarctions in the groups studied, A to F. (B) Facial corticobulbar tract (CBT) fibre distribution is shown in the upper medulla: dc=descending fibres; as=ascending fibres.
Additional clinicoradiological, clinicopathological, and neuroanatomical studies should help to further clarify the courses of central pathways, including the CBT, in humans.
Acknowledgments
This work was supported by a research grant for longevity sciences (110-05) from the Ministry of Health and Welfare.