Article Text

Statistics from Altmetric.com
Description
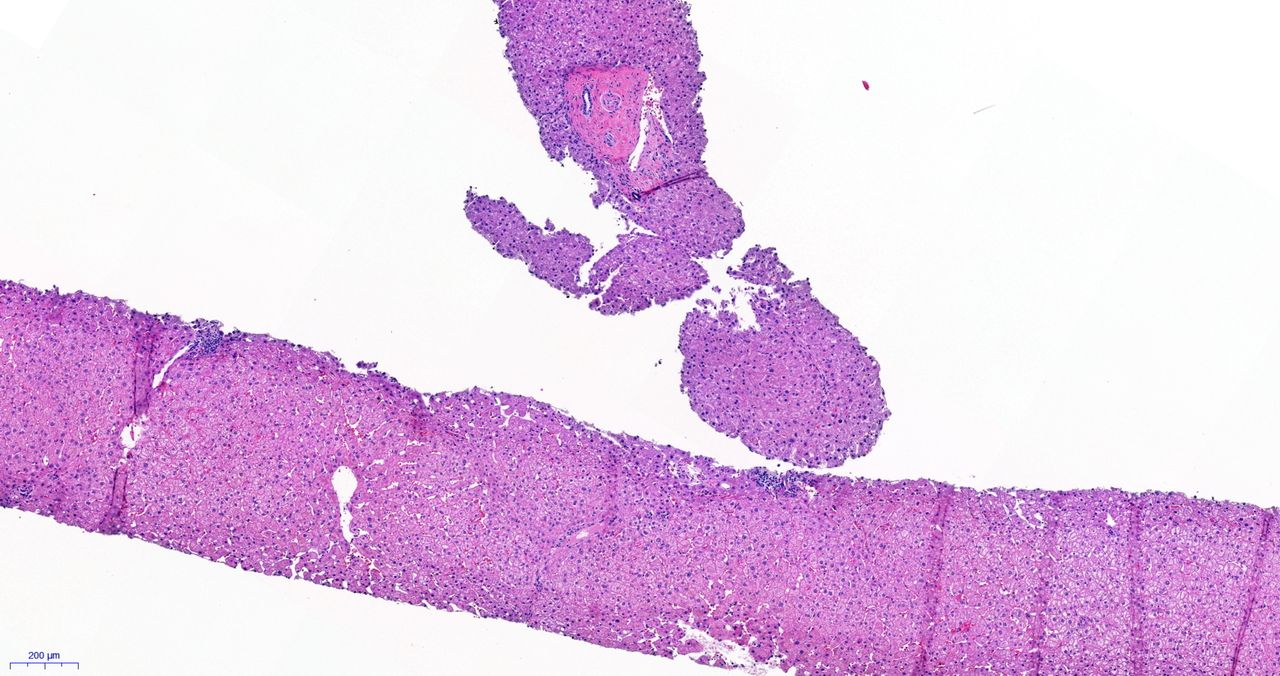
A 51-year-old female patient was diagnosed with primary biliary cholangitis (PBC) in 2012 and rheumafactor-positive, Anti-citrullinated protein antibodies (ACPA)-positive rheumatoid arthritis (RA) in 2013. The diagnosis of a PBC was confirmed by liver biopsy showing portal inflammatory infiltrates with non-suppurative inflammatory lesions of the biliary duct (figure 1). PBC has been treated with ursodeoxycholic acid since 2012.

Dense lymphocytic infiltrates in portal tracts affecting small portal bile ducts, moderate lobular infiltrates.
After diagnosis of RA (initial Disease Activity Score 28 (DAS 28)=6.43), therapy was initiated with leflunomide 20 mg/day and low-dose oral glucocorticoids, tapered from 20 mg/day to zero over 12 weeks. Remission was reached within 4 months (DAS 28=1.84). However, elevated transaminases were detected. As a consequence, leflunomide was switched to sulfasalazine in September 2013. After an increase of activity of RA under sulfasalazine, abatacept 750 mg every 4 weeks was added to treatment in January 2015. Under this treatment strategy remission was achieved in April 2015 and maintained thereafter (September 2017, DAS 28=2.27).
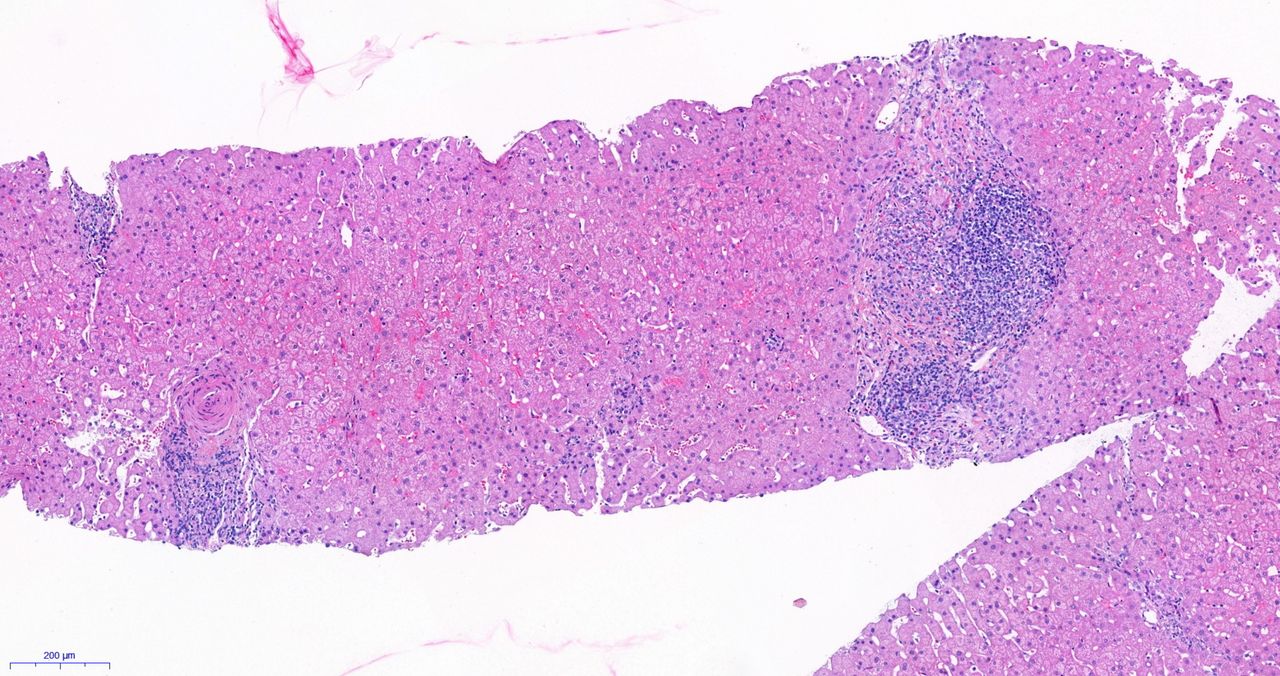
Liver stiffness as surrogate for fibrosis/cirrhosis was determined by elastography. It improved and normalised under treatment with sulfasalazine and abatacept (6.0 kPa in September 2013, 3.9 kPa in December 2016). Alkaline phosphatase and gamma-glutamyltransferase were elevated up to four times over the norm upon diagnosis of PBC. These enzymes showed, apart from transient elevation while leflunomide treatment, continuous improvement and finally normalised under treatment with abatacept and sulfasalazine (November 2017). In a control liver biopsy in September 2017 findings were improved, showing histologically only discrete portal and lobar inflammation without the typical pattern of a PBC (figure 2).
{kind=link}
{kind=link}
Regredient lymphocytic infiltrates, focal portal and periductal fibrosis without inflammation, preserved lobular architecture.
This case demonstrates improvement of PBC under therapy for RA with sulfasalazine and abatacept. The decision to use abatacept was supported by findings demonstrating participation of T cells in the pathogenesis of PBC1 and by Dhirapong et al2 who reported positive effects of therapy with abatacept in a mouse model for PBC.
Patient’s perspective
The diagnosis of PBC in 2012 and RA in 2013 was hard to cope with, especially when the side effects of leflunomide appeared and the sulfasalazine monotherapy did not show the wanted effect. Besides the knowledge of having an autoimmune disease of the liver, the everyday restriction caused by the temporary active RA was, apart from the need for oral glucocorticoids, which I was focused on in a negative way. With the well-tolerated, new treatment combination (sulfasalazine and abatacept), both diseases, PBC and RA, are fortunately in remission, which makes me look positively into my future.
Learning points
T cells play an important role in the pathogenesis of autoimmune diseases like primary biliary cholangitis (PBC) and rheumatoid arthritis.
Abatacept can be a significant treatment option in T cell-mediated diseases—further studies need to be made, especially for diseases like PBC, in which abatacept is not a recognised standard treatment.
Footnotes
Contributors FP and RBM: interpretation of data, writing of the manuscript, therapeutic decisions and monitoring of patient. DS: interpretation of data, writing of the manuscript, fibroscan and liver biopsy. JvK: interpretation of data and writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.