
Abstract
Introduction
D-Dimer (DD) has been described as a useful predictor of both morphologic changes in acute thoracic aortic dissection (TAD) and of TAD-associated mortality. This study analyzed the use of DD screening to screen patients with chest pain for acute (TAD) to determine if it improves diagnosis and cost effectiveness. This study also looked at the association of DD levels with diagnoses frequently seen in patients with dyspnea or chest pain.
Methods
At the Helios Hospital, Krefeld, the authors analyzed the data of all patients (n=1053, age (mean, SD) 62±19 years, 49% males) admitted for chest pain to the nonsurgical emergency department (ED) in February 2010. Chest pain was the second most frequent symptom causing 138 (13.1%) admissions, 102 of which had DD testing (Inniovance® D-Dimer Assay, Dade Behring/Siemens, Germany). To assess the diagnostic reliability of DD testing, the sensitivity, specificity, and odds ratio, including 95% confidence interval, were estimated.
Results
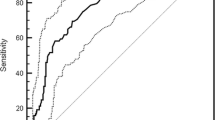
None of the patients admitted were found to have acute TAD. Had the authors used a computerized tomography (CT) scan to rule out TAD in every patient with chest pain, actual costs would have been €12,328. A restriction of CT scans to patients with elevated DD levels would have lowered costs to €5360. The actual costs were €670.30 for CT scans and €540.60 for DD tests. On analyzing the association with other diagnoses, both sensitivity and specificity were low, with the exception of pneumonia.
Conclusion
Owing to the low incidence of TAD, DD screening increases diagnostic efforts and costs but it remains unclear whether it would actually speed up TAD diagnosis. In a clinical setting DD did not help to discriminate other relevant diagnoses. Despite the high sensitivity of DD for aortic dissection published in the literature, the physician’s clinical judgment remains paramount.
Similar content being viewed by others


References
Courtney DM, Kline JA, Kabrhel C, et al. Clinical features from the history and physical examination that predict the presence or absence of pulmonary embolism in symptomatic emergency department patients: results of a prospective, multicenter study. Ann Emerg Med. 2010;55:307–315.e1.
Goldin Y, Pasvolsky O, Rogowski O, et al. The diagnostic yield of D-dimer in relation to time from symptom onset in patients evaluated for venous thromboembolism in the emergency medicine department. J Thromb Thrombolysis. 2011;31:1–5.
Kabrhel C, Mark Courtney D, Camargo CA Jr, et al. Factors associated with positive D-dimer results in patients evaluated for pulmonary embolism. Acad Emerg Med. 2010;17:589–597.
Norlin JM, Elf JL, Svensson PJ, Carlsson KS. A costeffectiveness analysis of diagnostic algorithms of deep vein thrombosis at the emergency department. Thromb Res. 2010;126:195–199.
Lemaire SA, Russell L. Epidemiology of thoracic aortic dissection. Nat Rev Cardiol. 2011;8:103–113.
Shimony A, Filion KB, Mottillo S, et al. Meta-analysis of usefulness of D-dimer to diagnose acute aortic dissection. Am J Cardiol. 2011;107:1227–1234.
Gruettner J, Henzler T, Sueselbeck T, et al. Clinical assessment of chest pain and guidelines for imaging. Eur J Radiol. 2011 Mar 9. [Epub ahead of print]
Khan IA, Nair CK. Clinical, diagnostic and management perspectives of aortic dissection. Chest. 2002;122:311–328.
Meszaros I, Morocz J, Szlavi J, et al. Epidemiology and clinicopathology of aortic dissection. Chest. 2000;117:1271–1278.
Friese KK, Steffens JC, Caputo GR, et al. Evaluation of painless aortic dissection with MR imaging. Am Heart J. 1991;122:1169–1173.
Khan IA, Vasavada BC, Sacchi TJ. Asymptomatic dissection of the ascending aorta: diagnosis by transesophageal echocardiography. Am J Emerg Med. 1999;17:172–173.
Khurana B, Goorahoo P, Friedman SA. Silent aortic dissection with hemopericardium: diagnosis by computerized tomography. Chest. 1988;93:652–653.
Eggebrecht H, Naber CK, Bruch C, et al. Value of plasma fibrin D-dimers for detection of acute aortic dissection. J Am Coll Cardiol 2004;44:804–809.
Iyano K, Kawada T, Aiba M, et al. Correlation of hemostatic molecular markers and morphology of the residual false lumen in chronic aortic dissection. Ann Thorac Cardiovasc Surg. 2004;10:106–112.
Nomura F, Tamura K, Yoshitatsu M, et al. Changes in coagulation condition, cytokine, adhesion molecule after repair of type A aortic dissection. Eur J Cardiothorac Surg. 2004;26:348–350.
Weber T, Hogler S, Auer J, et al. D-dimer in acute aortic dissection. Chest. 2003;123:1375–1378.
Suzuki T, Distante A, Zizza A, et al. Diagnosis of acute aortic dissection by D-dimer: the International Registry of Acute Aortic Dissection Substudy on Biomarkers (IRAD-Bio) experience. Circulation. 2009;119:2702–2707.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moysidis, T., Lohmann, M., Lutkewitz, S. et al. Cost associated with D-Dimer screening for acute aortic dissection. Adv Therapy 28, 1038–1044 (2011). https://doi.org/10.1007/s12325-011-0069-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-011-0069-2