Article Text

Statistics from Altmetric.com
Description
A 30-year-old male patient with a history of malignant, metastatic paraganglioma presented with a rapidly enlarging, expansile left calvarial mass. CT and ultrasound imaging demonstrated a 60×46×31 mm soft-tissue lesion centred on the left frontal bone which was markedly hypervascular (figure 1A,B).
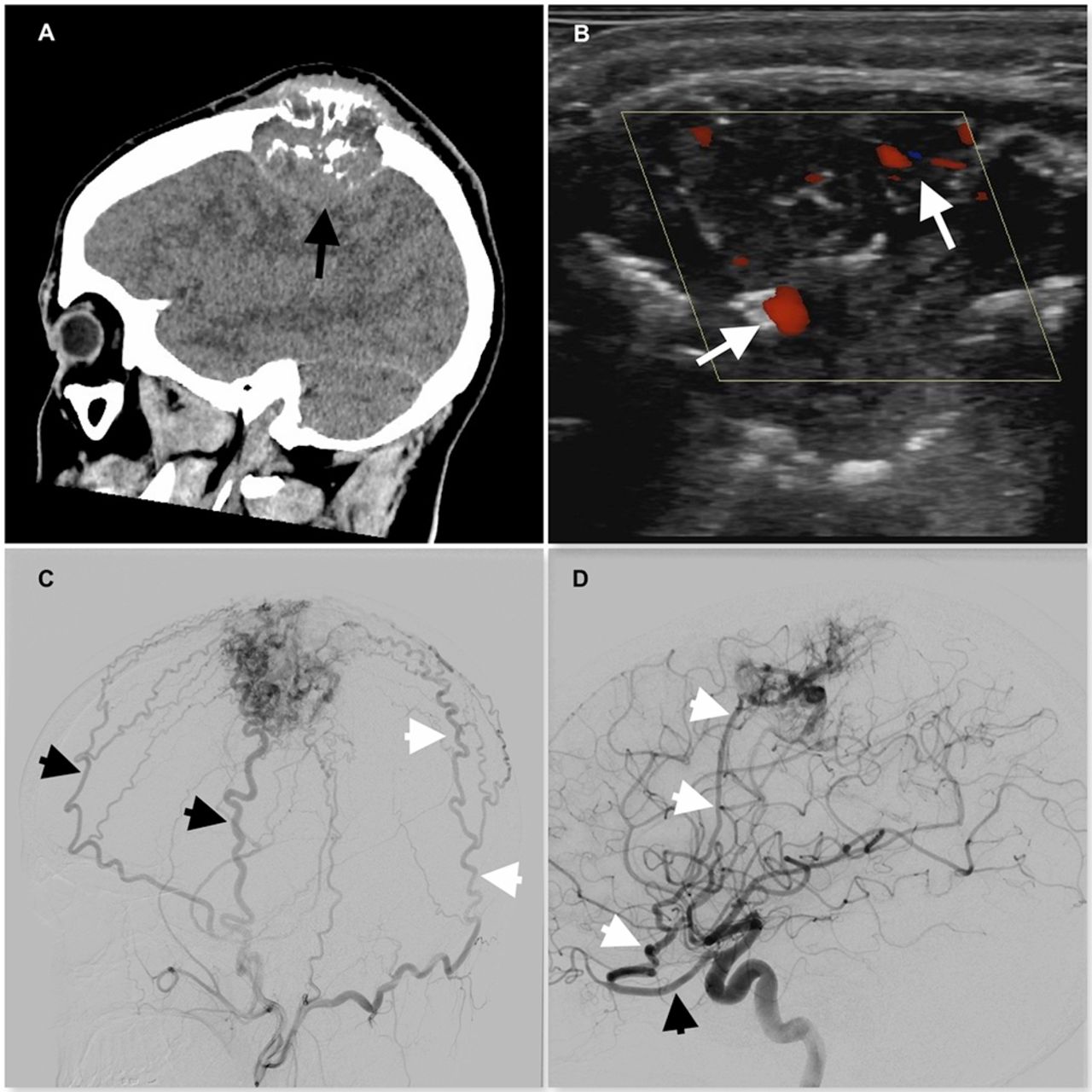
(A) non-contrast CT demonstrating the left-sided expansile calvarial lesion with osseous destruction and frontal lobe compression (black arrow). (B) Colour flow Doppler ultrasound of the lesion demonstrating pronounced hypervascularity (white arrows). (C) Lateral left external carotid artery DSA demonstrating extensive superficial scalp supply to the lesion from multiple, enlarged superficial temporal artery (black arrowheads) and occipital artery (white arrowheads) branches. (D) Lateral left internal carotid artery DSA demonstrating deep dural arterial supply to the lesion from the MMA (white arrowheads) originating from the ophthalmic artery (black arrowhead). DSA, digital subtraction angiogram; MMA, middle meningeal artery.
A cerebral digital subtraction angiogram (DSA) was then performed in order to further delineate the arterial blood supply to the lesion (figure 1C,D). This DSA demonstrated a significant superficial, scalp supply to the lesion via innumerable enlarged branches of the occipital and superficial temporal arteries and a deep, dural supply via the dilated middle meningeal artery (MMA), unusually arising from the ophthalmic artery in this patient.
Preoperative embolisation was undertaken prior to surgical excision to lessen intraoperative blood loss. The diffuse nature of the superficial scalp supply to the lesion with multiple feeding arterial branches meant it was a poor target for transarterial embolisation. Therefore, direct percutaneous glue embolisation was performed with five glue injections resulting in near total occlusion of the superficial scalp arterial supply (figure 2A). A 6 Fr Envoy guide catheter (DePuy Synthes, West Chester, Pennsylvania, USA) was then positioned in the left internal carotid artery and a Headway Duo microcatheter (Microvention, Tustin, California, USA) was negotiated into the MMA via its aberrant origin from the ophthalmic artery (figure 2B). Glue embolisation of the MMA was then performed via the Headway Duo without complication (figure 2C,D). The patient went on to have successful surgical excision of the lesion with moderate intraoperative blood loss of 1200 mL, followed by titanium cranioplasty.

{kind=link}
{kind=link}
(A) Antero-posterior radiograph post ultrasound and fluoroscopic-guided percutaneous embolisation demonstrates the puncture needle within the lesion (black arrow) and large glue cast (white arrow). (B) Magnified lateral left internal carotid artery DSA demonstrating negotiation of microwire and microcatheter (white arrowhead) into the MMA arising from the ophthalmic artery (black arrowhead). (C and D) Subtracted (C) and unsubtracted (D) lateral left common carotid artery DSA images following percutaneous and transarterial glue embolisation of the left calvarial paraganglioma metastases demonstrate significant reduction in arterial blood flow to the lesion in comparison to pre-embolisation DSA (figure 1C,D). The embolised MMA stump (white arrowhead) may be visualised with no distal flow with only minimal residual supply from superficial temporal artery branches (black arrowheads). DSA, digital subtraction angiogram; MMA, middle meningeal artery.
Paragangliomas are rare neoplasms consisting of neuroendocrine cells derived from the embryonic neural crest. The majority are benign, with malignant paragangliomas occurring at an estimated 93 cases per 400 million persons.1 Paraganglioma metastases to the calvarium are extremely rare, with only two cases described in the literature.2 In common with primary paragangliomas, paraganglioma metastases are often extremely hypervascular meaning preoperative embolisation can prevent significant haemorrhage during surgical excision. This case demonstrates that even with complex, dual supply from superficial scalp and deep dural arteries, successful preoperative embolisation may be performed using unconventional access routes.
Learning points
Preoperative embolisation of hypervascular, calvarial paraganglioma metastases may lessen the risk of significant haemorrhage during surgical excision.
Superficial scalp arterial supply to these lesions may be best embolised via a direct percutaneous approach allowing better glue penetration into the lesion.
Knowledge of variant anatomy, such as the aberrant origin of the middle meningeal artery from the ophthalmic artery in this paper, is essential for safe and effective embolisation strategies
References
Footnotes
Contributors NJ as primary author with revisions by MTC and drafting by WM and AB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.