Article Text

Statistics from Altmetric.com
Description
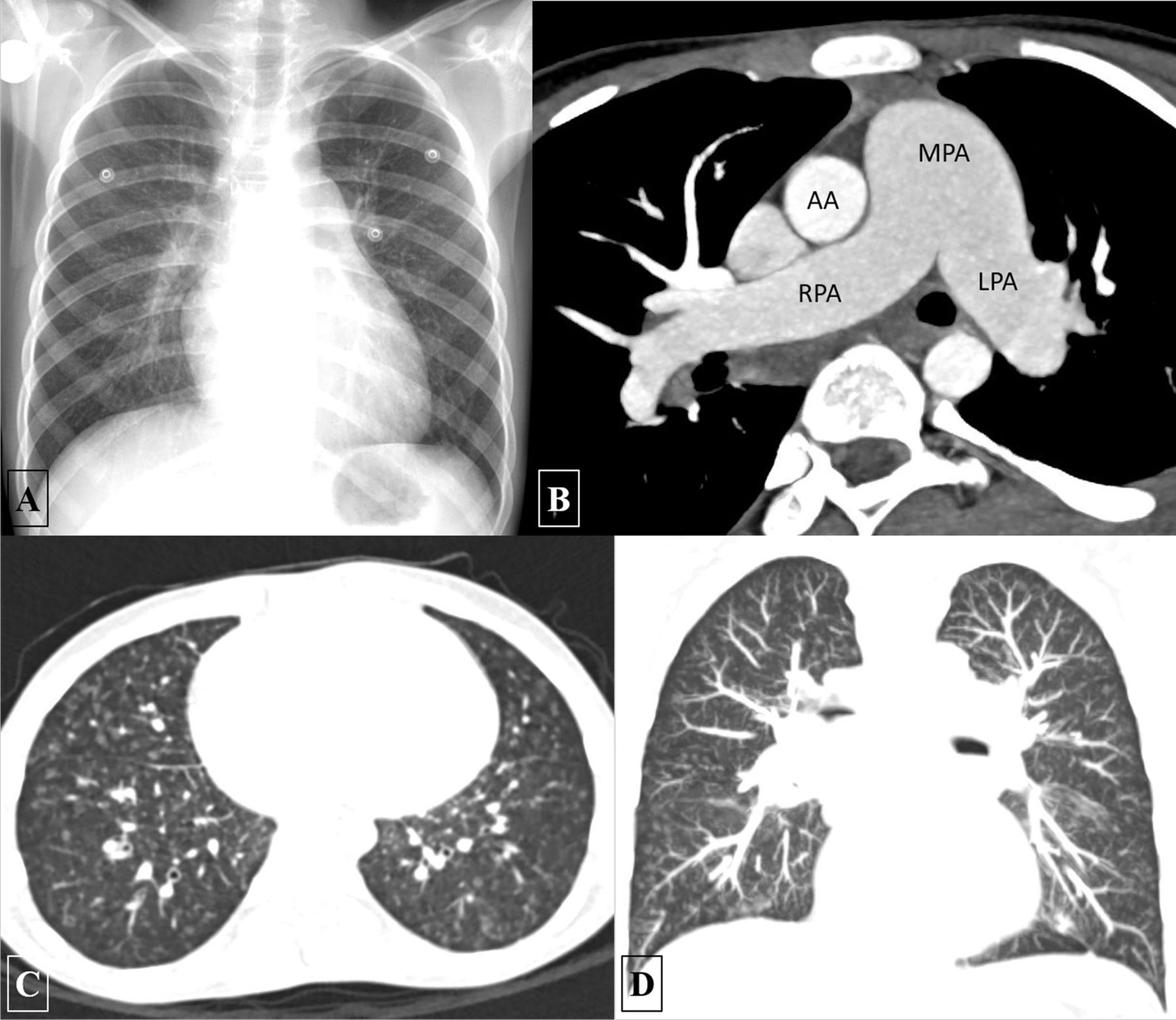
Pulmonary capillary haemangiomatosis (PCH) is a rare cause of pulmonary hypertension which poses a considerable diagnostic challenge. Here, we describe the case of a 14-year-old boy with gradually progressive exertional dyspnoea and cough for past 4 months. Frontal chest radiograph demonstrated prominent pulmonary artery segment with diffuse nodular opacities in bilateral lung fields (figure 1A). CT angiography was performed to diagnose the aetiology of pulmonary artery hypertension. It revealed dilated central pulmonary arteries (figure 1B) with multiple ill-defined centrilobular nodules diffusely distributed in both lungs (figure 1C,D). No interlobular septal thickening, pulmonary thromboembolism, pleural effusion or any intracardiac/extracardiac shunt was seen. A provisional diagnosis of PCH was made which was subsequently confirmed on a lung biopsy.
{kind=link}
Frontal chest radiograph (A) revealing prominent pulmonary artery segment with reticulonodular opacities predominantly involving the lower zones. No Kerley lines were noted. Axial maximum intensity projection images of CT angiography (B) showing dilated MPA, RPA and LPA. No intraluminal filling defects are seen. Axial (C) and coronal (D) lung window images showing the presence of diffuse, ill-defined, centrilobular nodules in both lungs. No septal thickening or any other parenchymal lesion noted. AA, ascending aorta; LPA, left pulmonary artery; MPA, main pulmonary artery; RPA, right pulmonary artery.
Clinical presentation of PCH is non-specific and generally confused with primary pulmonary hypertension and pulmonary veno-occlusive disease (PVOD).1 2 Characteristic imaging findings in PCH include the presence of diffuse, ill-defined, centrilobular nodules or ground-glass opacities with scarce septal lines and the presence of haemorrhagic pleural effusions. In contrast, septal lines are frequently encountered in PVOD while haemorrhagic effusions are extremely uncommon.1 Correct diagnosis is imperative as standard vasodilator therapy or prostacyclin infusion, a mainstay in the treatment of pulmonary hypertension, can result in sudden respiratory distress and death (due to florid pulmonary oedema) in these patients.3 Treatment with recombinant interferon-alpha-2a has been shown to lead to stabilisation of disease or even improvement in a few reported cases. However, lung transplantation remains the only definitive treatment for PCH.
Learning points
Pulmonary capillary haemangiomatosis (PCH) is an uncommon cause of pulmonary hypertension with non-specific clinical presentation, overlapping with primary pulmonary hypertension and pulmonary veno-occlusive disease.
Characteristic imaging findings include the presence of diffuse, ill-defined, centrilobular nodules or ground-glass opacities with scarce septal lines and the presence of haemorrhagic pleural effusions.
Precise diagnosis is crucial as a standard treatment of pulmonary hypertension, including vasodilator therapy or prostacyclin infusion, can have catastrophic consequences in these patients.
Footnotes
AS, NNP and SK contributed equally.
Contributors AS, NNP and SK: participated sufficiently in the conception of the idea, development of the intellectual content, design, writing and final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.