Article Text

Statistics from Altmetric.com
Description
A 38-year-old man with a medical history of hepatitis C presented with a 2-day pruritic rash. It started on his back and generalised within 2 days. The patient had been on vancomycin for the last 3 weeks due to a recent diagnosis of osteomyelitis. He was not taking other medications. On physical examination, a diffuse blanching maculopapular exanthema was noted (figure 1A and B) associated to facial angioedema and palpable axillary and inguinal lymph nodes. Laboratory evaluation was relevant for leucocytosis with neutrophilia and eosinophilia, mild elevation of liver function tests and peripheral blood smear revealing atypical lymphocytes (figure 2). Skin biopsy demonstrated superficial perivascular dermatitis with papillary dermal oedema (figure 3). Diagnosis of drug reaction with eosinophilia and systemic symptoms (DRESS) was made. Vancomycin was suspended and daptomycin was initiated. He also received treatment with high-dose antihistamines and systemic corticosteroids. Follow-up showed resolution of the rash.
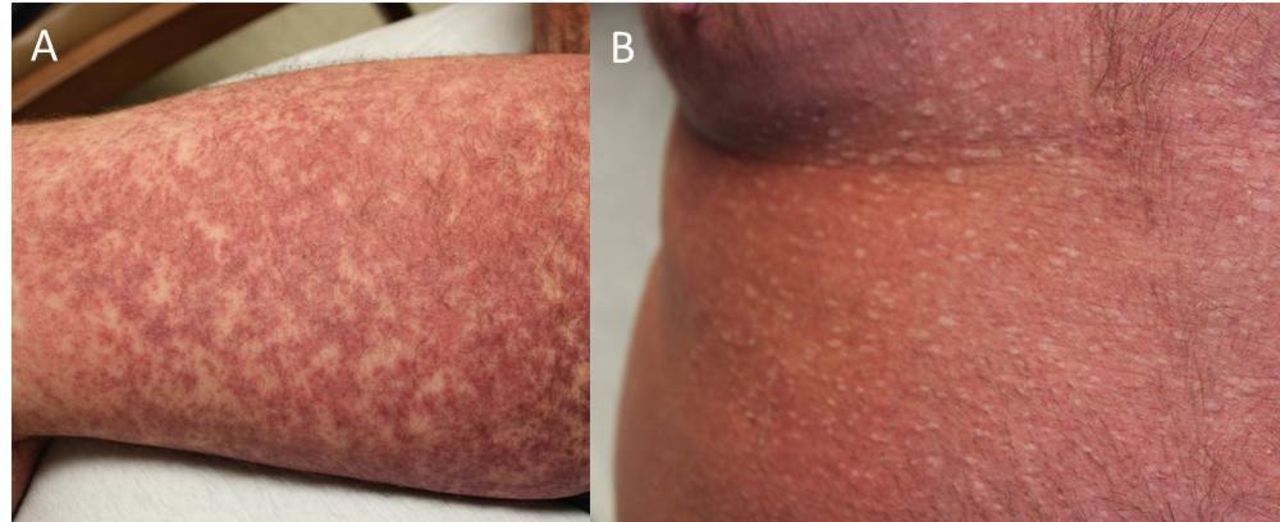
Diffuse blanching maculopapular exanthema located in thigh (A) and abdomen (B).

Peripheral blood smear showing atypical lymphocytes.

{kind=link}
{kind=link}
{kind=link}
Skin biopsy demonstrating superficial perivascular dermatitis with papillary dermal oedema.
DRESS syndrome is a rare but potentially life-threatening condition characterised by a delayed multisystem compromise following the administration of a drug.1 Symptoms include rash, fever, haematological abnormalities (ie, leucocytosis, eosinophilia and atypical lymphocytosis), lymphadenopathy and internal organ involvement, most commonly being involved the liver or kidneys.2 The rash is usually diffuse and maculopapular, but other dermatological presentations are common, including vesicles, pustules and bullae.1 DRESS syndrome most commonly occurs after treatment with anticonvulsants, but it also occurs with other types of drugs including vancomycin. It typically develops 2–6 weeks after the initiation of the drug.3 There are no validated diagnostic criteria, but the RegiSCAR score system is the most commonly used. The following criteria are included: fever ≥38.5°C, enlarged lymph nodes (>1 cm size in at least two sites), eosinophilia (≥700 or ≥10%), atypical lymphocytes, rash (with scaling, angioedema, purpura, infiltration) which comprises ≥50% of body surface area and involvement of at least one internal organ.2 Histopathological analysis can reveal a combination of lymphocytic exocytosis, epidermal spongiosis, interface vacuolisation, papillary oedema (seen in our patient), and perivascular lymphocytic and eosinophilic infiltration.2 Stopping the triggering drug is the most important step when managing patients with DRESS syndrome. Treatment also comprises supportive measures, corticosteroids and immunosuppressants.3
Learning points
Drug reaction with eosinophilia and systemic symptoms syndrome is a potentially fatal reaction to drugs.
Symptoms include rash, fever, haematological abnormalities and organ involvement.
It most commonly occurs secondary to anticonvulsants but can also be secondary to other type of drugs, including vancomycin.
Footnotes
Contributors NC-P: reporting, conception and design, analysis and interpretation of data. AP: reporting, conception and design, acquisition of data or analysis and interpretation of data. GY: planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data. AG-E: planning, conduct, reporting, conception and design, acquisition of data or analysis and interpretation of data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.