Article Text

Statistics from Altmetric.com
Description
Traumatised teeth usually develop pulp canal obliterations and are characterised by radiographic loss of pulp space and yellowish discoloration of clinical crown.1 2 The American Association of Endodontists included teeth with radiographic indiscernible root canals requiring treatment in high difficulty criteria.3 Proper debridement, disinfection and obturation of root canal is difficult in such cases thus compromising root canal treatment. This article presents case of pulp canal obliteration of maxillary central incisor that was managed with usage of cone beam CT (CBCT), microscopes, periodic radiographs and small sized hand files which helped in achieving patency to the pulp chamber and root canal.
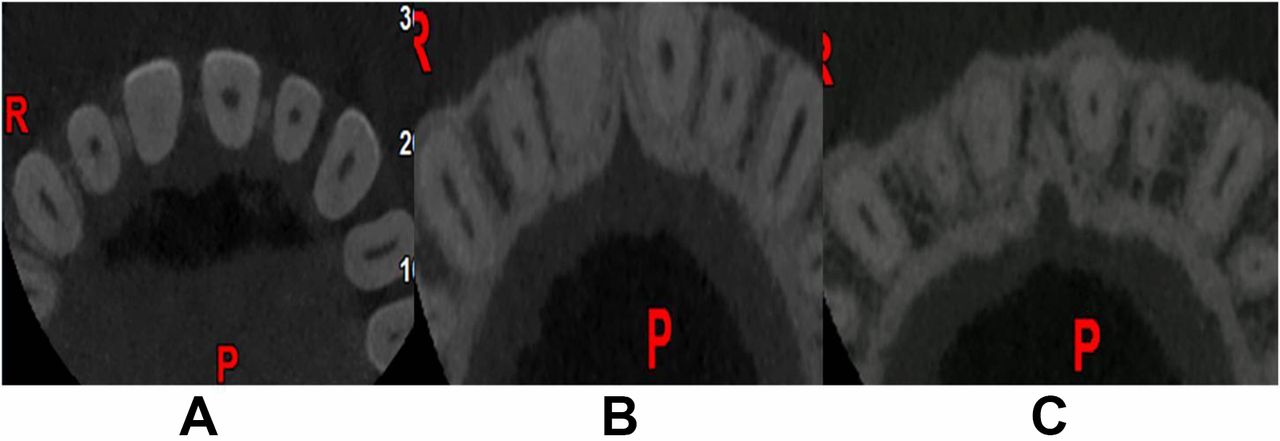
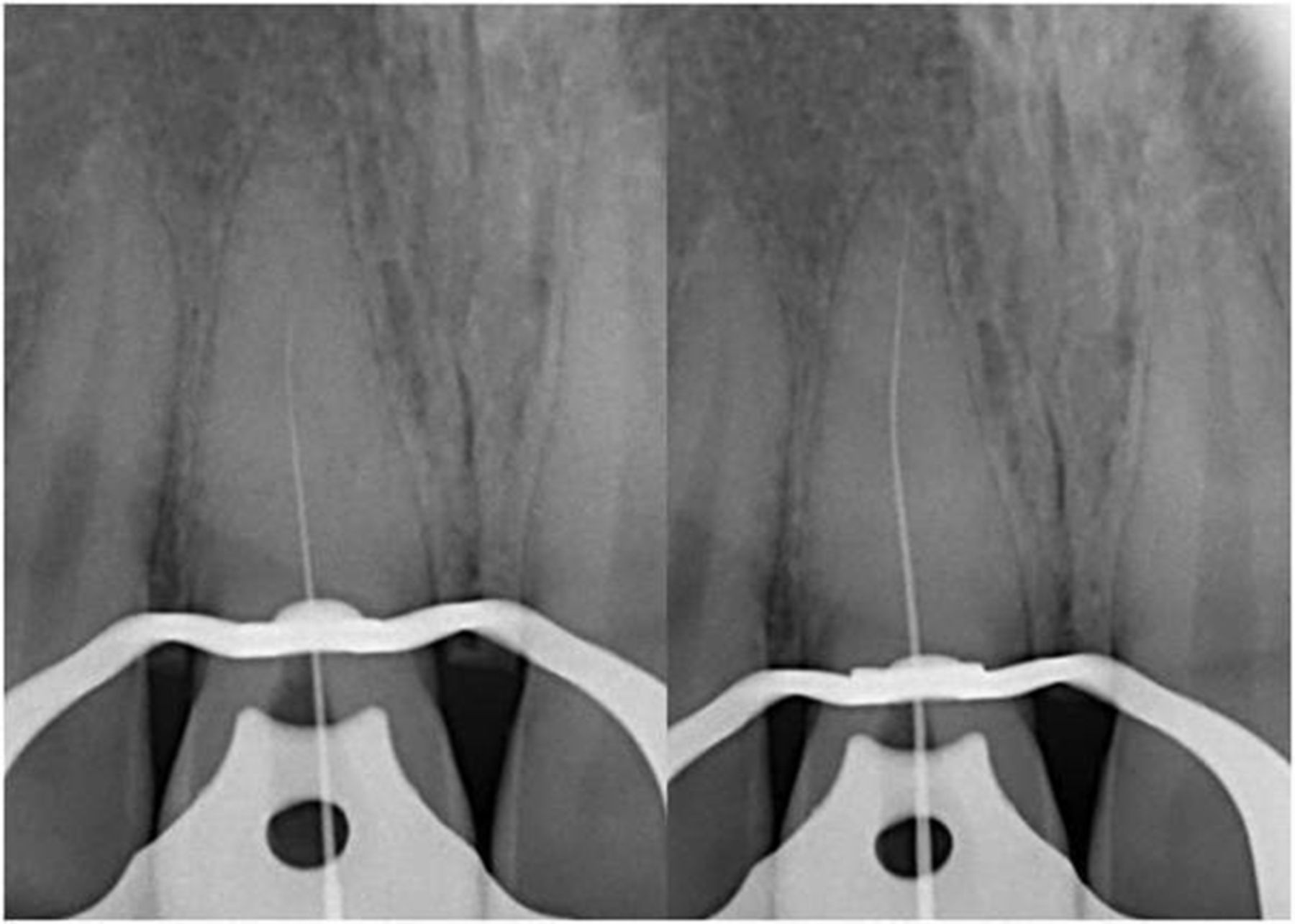
A 35 year old male patient reported with pain in upper front region of jaw since 3 months. The patient gave history of trauma 3 years ago when he met with an accident, thereafter he noticed gradual change in the transparency of the crown but there was no pain. The patient elicited history of trauma again on the same tooth 3 months back when he was playing games after which he developed pain on biting. Pissiotis et al 4 showed that repeated traumatic episodes have an effect on pulpal healing which increases the risk of developing pulp canal obliteration and pulp necrosis. Intraoral examination revealed discoloration of tooth 11 with tenderness to vertical percussion. Thermal and electric pulp response was negative with tooth 11 whereas adjacent teeth showed normal response. Preoperative radiograph revealed partial pulp canal obliteration with periodontal ligament widening in the apical region (figure 1). CBCT (Carestream, Rochester, NY) was taken to check the continuity and patency of canal in different levels of root. Axial section of coronal, middle and apical third of root revealed partially obliterated pulp chamber and pulp canal (figure 2). Diagnosis of symptomatic apical periodontitis with partial obliteration of the pulp canal was made and non surgical root canal treatment was advised to the patient. History of trauma 3 months ago may be the reason for symptomatic apical periodontitis which represents inflammation of apical periodontium producing a painful response to biting or percussion. This may or may not be associated with radiographic changes.5 After obtaining consent, the tooth was anaesthetised and isolated under rubber dam. Access cavity was prepared close to incisal edge using extended shank round burs (Brasseler, Savannah, GA, USA) and ultrasonic BUC 1 tips (SybronEndo, Orange, California, USA) which facilitated straight line access.6 Scouting of the root canal orifices was done using a DG 16 explorer and visualised under surgical operating microscope (Carl Zeiss Surgical, Oberkochen, Germany) (figure 3). Size 8 K file (Mani, Japan) was introduced into the root canal with which obliteration was felt in the middle third. C+ files (Dentsply, Tulsa, OK, USA) have stronger buckling resistance compared with K files and provide easy negotiation and access to apical third of root. Size 8 C+ file was used in watch winding motion with minimal vertical pressure and regularly replaced before signs of fatigue occurred along with copious irrigation of 17% EDTA to reach till the apex. Working length was measured using an electronic apex locator (Root ZX II, J Morita, Tustin, CA) and confirmed radiographically (figure 4). The root canal was prepared by crown down approach7 using ProTaper Next rotary files to size X2 (Dentsply Maillefer, USA) with copious amount of 5.25% sodium hypochlorite (Cmident India, Delhi) as irrigant during instrumentation. Master cone radiograph confirmed the apical extent of gutta percha and obturation was completed using ProTaper Next X2 gutta-percha (Dentsply Maillefer) and AH Plus (Dentsply Maillefer) as endodontic sealer. The follow up was made after 3 months where the patient was asymptomatic without any tenderness (figure 5).

Preoperative photograph and radiograph showing crown discoloration and pulp canal obliteration.
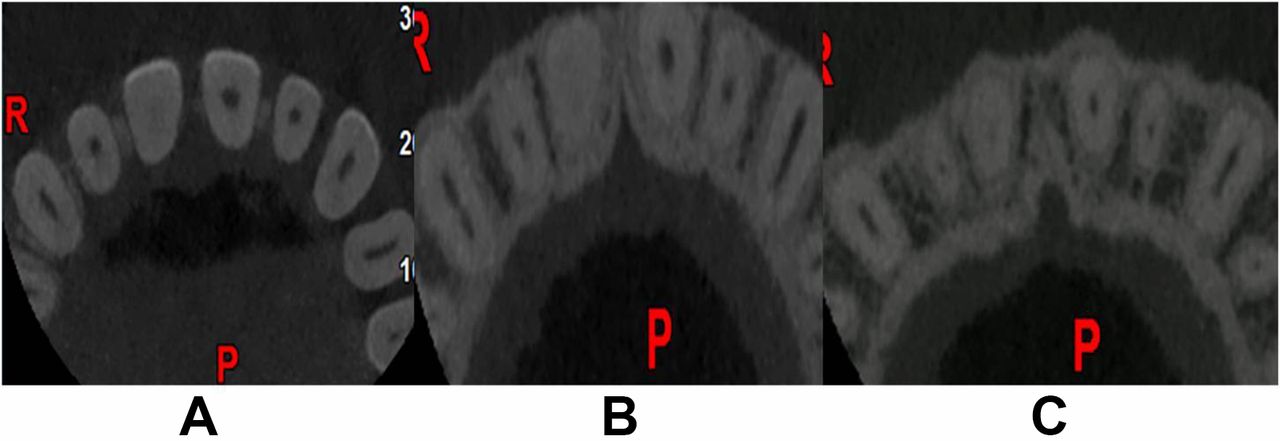
Cone beam CT (CBCT) axial images. (A) Coronal third section showing partially obliterated pulp chamber. (B) Middle third section showing partially obliterated pulp canal. (C) Apical third section showing partially obliterated pulp canal.

Access cavity preparation showing incisal preparation and straight line access.

Periodic radiographs showing working length determination.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Three-month postoperative radiograph.
Learning points
Radiographic obliteration of pulp space does not imply an absence of pulp tissue or space clinically.
Clinical symptoms or definite radiographic findings suggestive of periapical disease are indications of root canal treatment.
Diagnostic aids like cone beam CT, operating microscopes and proper armamentarium are the requisites to overcome the difficulties posed by pulp canal obliterations.
Footnotes
Contributors AL and AP have done the case. DKS and KE prepared the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.