Article Text

Statistics from Altmetric.com
Description
Foreign body ingestion is a common occurrence. Although over 80% of ingestions resolve spontaneously, approximately 1% of cases will require open surgical intervention. We present a rare case of foreign body ingestion in an 18-year-old man causing distal mechanical small bowel obstruction, requiring exploratory laparotomy and enterotomy.
An 18-year-old man with no significant medical history and no previous abdominal operations presented to a regional hospital with a 5-day history of persistent nausea, vomiting, absolute constipation and generalised abdominal pain. On clinical examination, he was tachycardic (116 beats/min) with a low-grade temperature (37.8°C), and had abdominal distension with central abdominal guarding. Plain films showed dilated loops of small bowel, consistent with small bowel obstruction. White cell count was 7.5×109/L and C reactive protein was 74 mg/L.
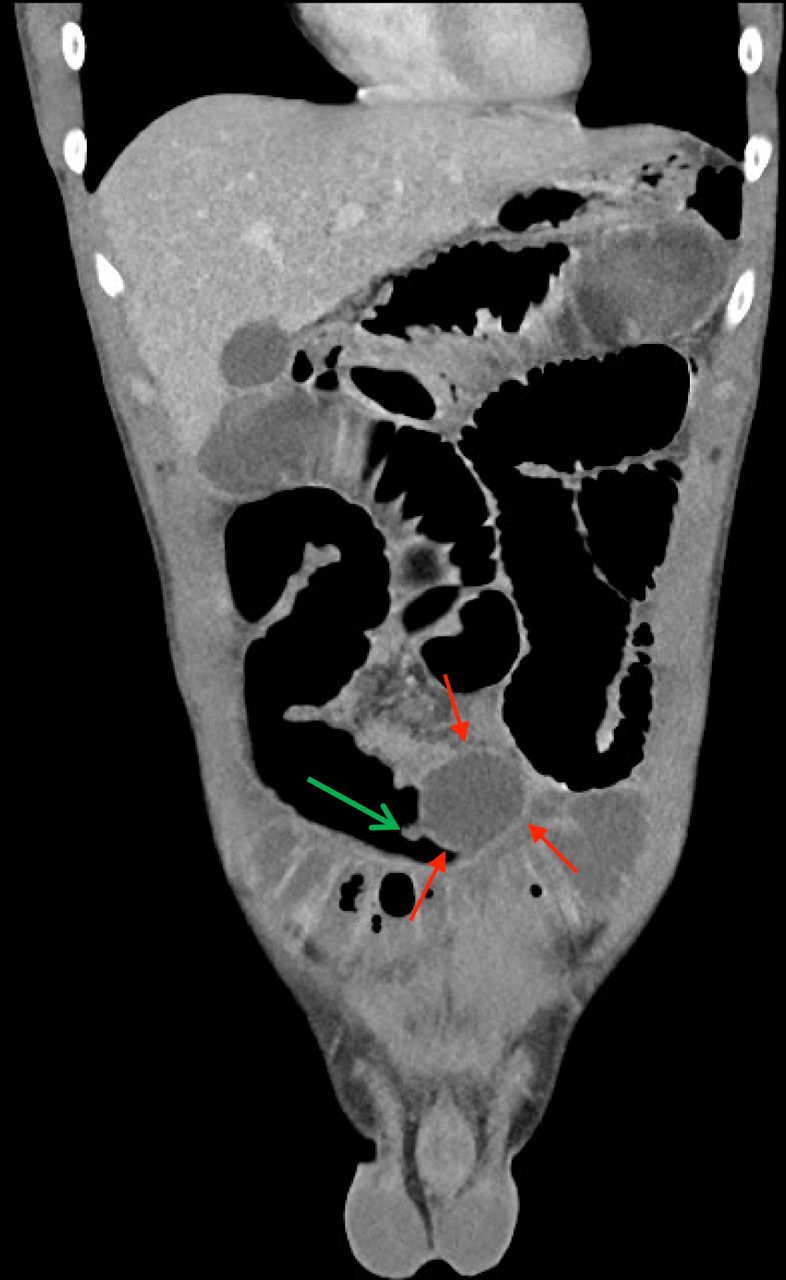
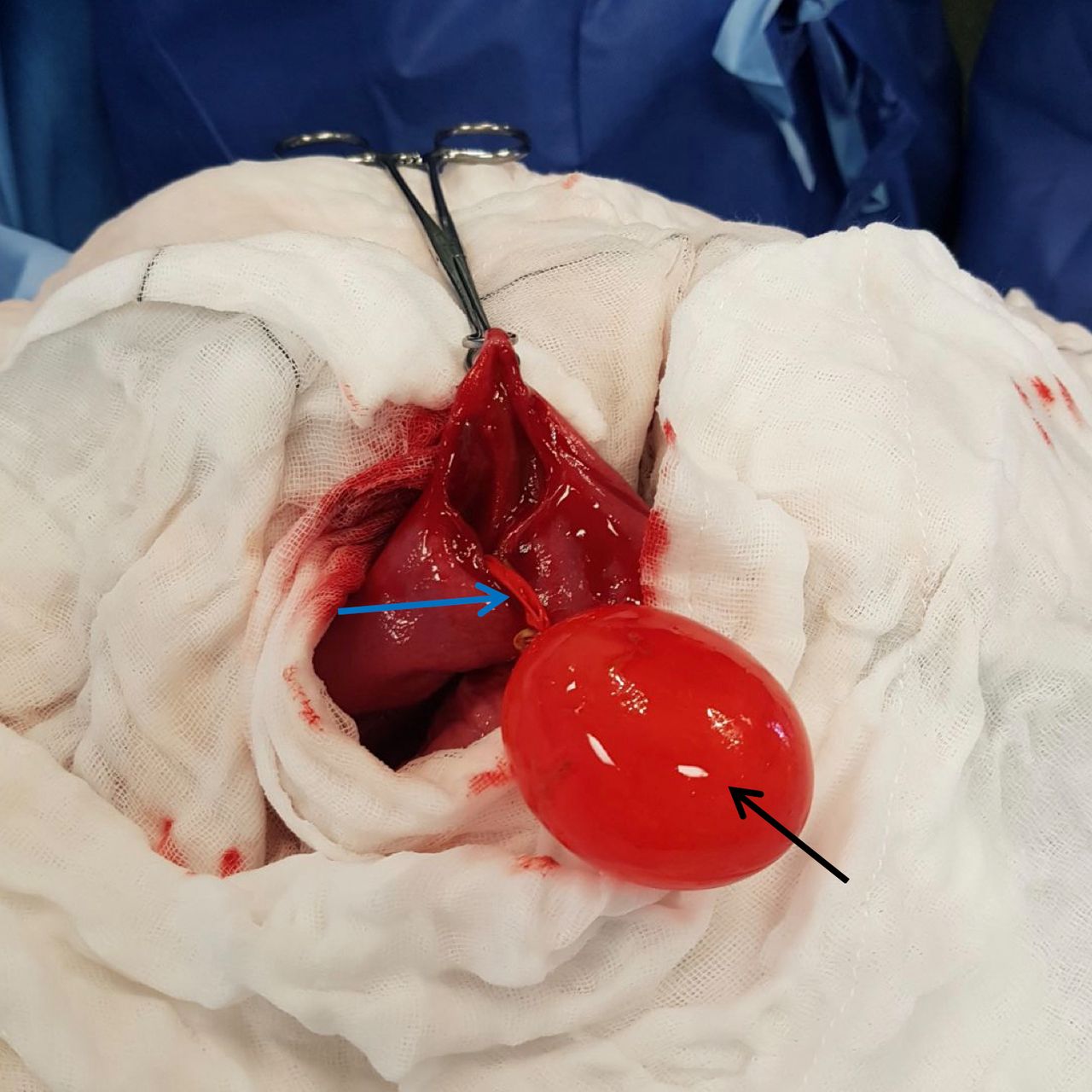
Subsequent evaluation with a CT scan demonstrated appearance of small bowel obstruction with at least one transition point in the left lower abdomen, with features concerning for internal herniation or mesenteric torsion resulting in closed loop obstruction. No foreign objects were seen at the initial reporting of imaging. A nasogastric tube was placed and an emergency explorative laparotomy was performed for concerns of closed loop bowel obstruction. Intraoperatively, small bowel dilatation was found throughout, up to the distal ileum. A soft, fluctuant and intraluminally mobile mass of approximately 4 cm in length was palpated in the distal ileum (figure 1). The mass was causing severe obstruction, and the bowel distal to this was collapsed. Enterotomy revealed a water-filled rubber balloon (figure 2). No history of foreign body ingestion was given by the patient on repeat assessments postoperatively. Given the density of the water balloon, only on retrospective review of the initial CT imaging was the foreign body identified (figure 3). The patient was discharged home after tolerating enteral nutrition and outpatient psychiatry review organised.

Intraoperative photo showing small bowel dilatation (green arrow) and soft fluctuant mass in the terminal ileum (red arrow).

Intraoperative photo showing water-filled rubber balloon (black arrow) and the tail of the balloon with a string attached (blue arrow).
{kind=link}
{kind=link}
{kind=link}
Coronal CT scan of the abdomen showing a radiolucent balloon in the distal ileum (red arrow) with balloon tail (green arrow).
Foreign body ingestion occurs primarily in young children between the ages of 6 months and 3 years, although ingestions can also present in other settings such as intentional ingestion in psychiatric patients or prison inmates.
The diagnosis of foreign body ingestion is primarily made clinically, although a history of foreign body ingestion may not always be available. Radiopaque objects can be localised and identified via biplanar radiographs, but radiolucent ones can evade timely diagnosis if a clinical history is lacking. Distal obstruction occurs in less than 10% of cases, where the most common point of impaction is the ileocaecal valve. Complications of foreign body ingestion include ulcer formation, mucosal laceration, perforation, intestinal obstruction, fistula formation and bacteraemia.1
Urgent intervention to remove a foreign body is indicated in certain situations such as airway compromise, oesophageal obstruction, signs and symptoms of intestinal inflammation or obstruction, or if the foreign object is sharp, long, consists of magnets, superabsorbent polymer or batteries. Over 80% of ingestions resolve spontaneously and pass without a need for intervention.2 In 20% of cases, endoscopic intervention is indicated. Less than 1% of ingested foreign bodies require open surgical intervention.2
Learning points
Foreign body ingestion is a common occurrence, and although few cases require open surgical intervention, urgent surgical removal is indicated in certain situations such as bowel obstruction/inflammation.
A high index of suspicion is required as the diagnosis is primarily made clinically.
Radiolucent objects may not be localised on radiographic investigations and a reliable history is not always available.
Complications of foreign body ingestion include ulcer formation, mucosal laceration, perforation, intestinal obstruction, fistula formation and bacteraemia.
Footnotes
Contributors ZAZ: writing of paper. DLCW: study design. TMAA: supervision and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.