Article Text

Statistics from Altmetric.com
Description
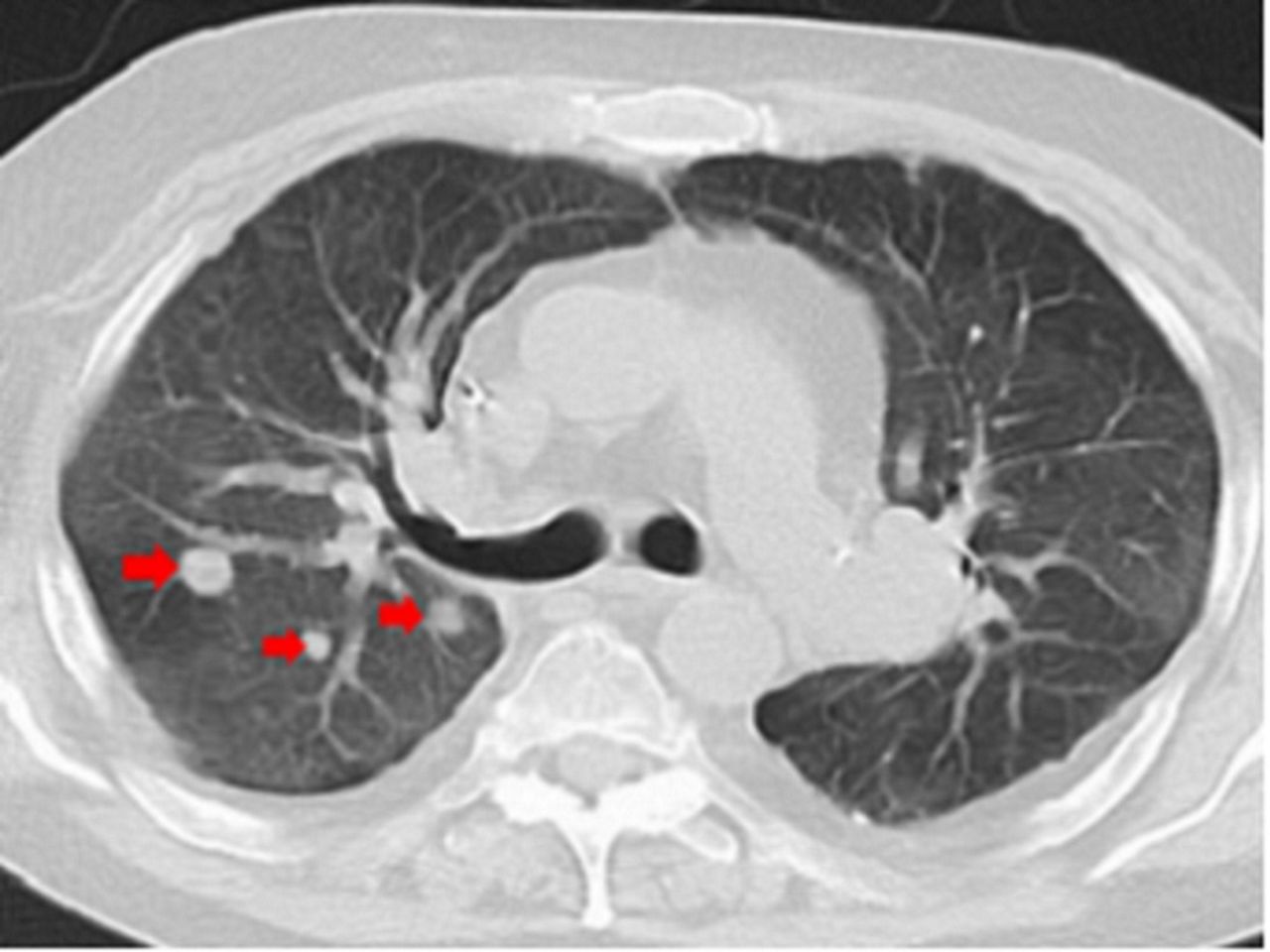
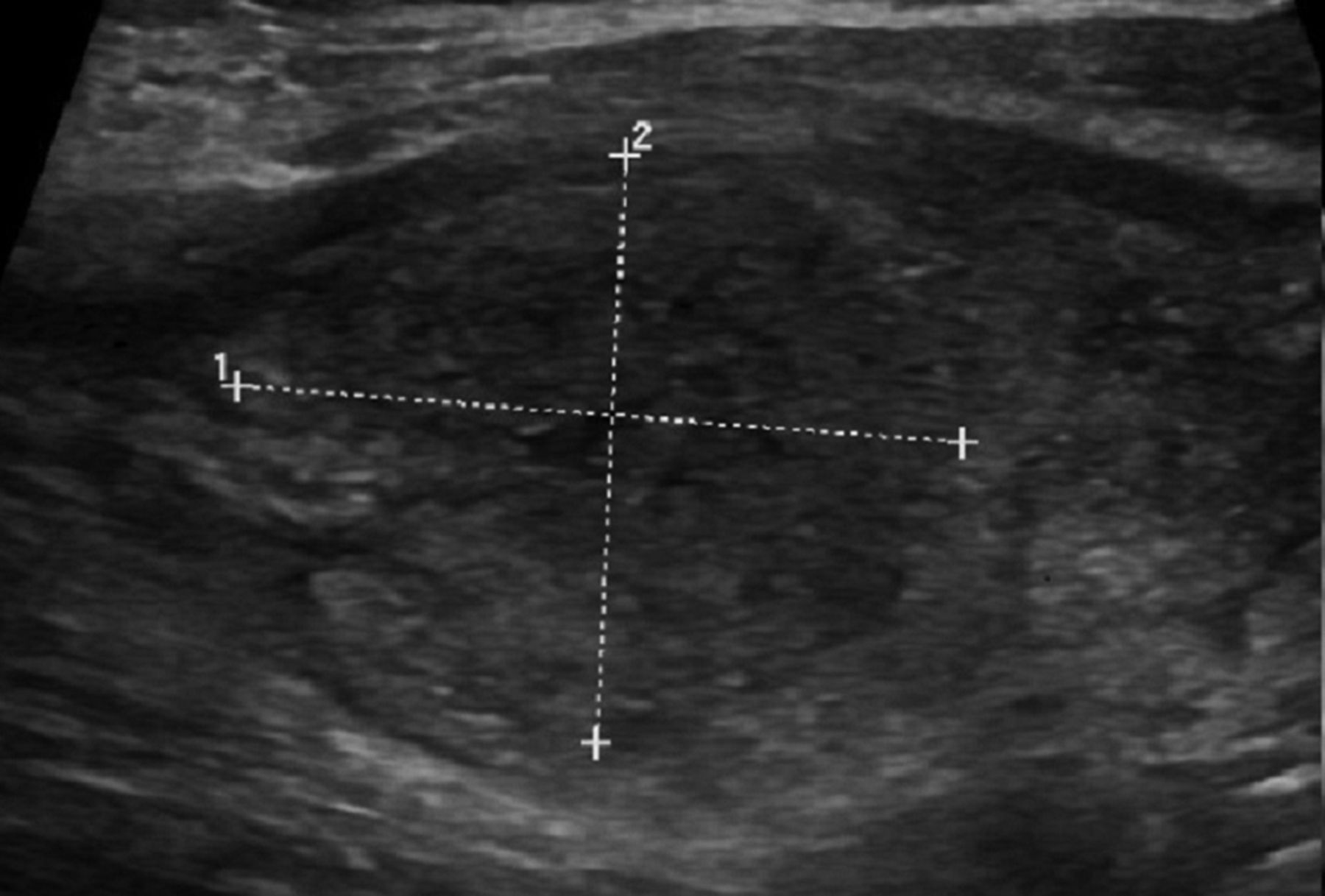
A 59-year-old man was admitted with 3 weeks of worsening shortness of breath 18 months after receiving a bilateral lung transplant for idiopathic pulmonary fibrosis. His immunosuppression included tacrolimus, everolimus and low-dose prednisone with no antifungal prophylaxis at the time of admission. CT chest revealed multiple, bilateral pulmonary nodules (figure 1—red arrows). CT-guided biopsy revealed fungal hyphae (figure 2). The initial CT and ultrasound of the neck at the onset of sore throat was negative; however, repeat CT neck for evolving neck pain and dysphasia during hospital course showed a mass-like lesion in the right thyroid lobe with extensive surrounding inflammatory changes (figure 3—green arrow). The lesion was also visualised on ultrasound, where it appeared as a hypoechoic solitary nodule (figure 4). Laboratory evaluation revealed hyperthyroidism, with a Thyroid Stimulating Hormone (TSH) of <0.01 µIU/mL (normal: 0.35–4.94 µIU/mL) and a free T4 of 2.72 ng/dL (normal: 0.70–1.48 ng/dL). The patient was initiated on dual antifungal therapy with liposomal amphotericin and posaconazole, resulting in rapid resolution of neck pain. However, repeat CT neck 2 weeks after revealed a thyroid abscess in the right lobe, and subsequently the patient underwent right thyroid lobectomy and isthmusectomy. Surgical debridement of the thyroid abscess revealed fungal hyphae; thus, confirming the diagnosis of fungal thyroiditis (figure 5). A specific fungal pathogen was never successfully cultured from our patient. He was treated for presumed Aspergillus infection, the most common etiology of fungal thyroiditis, with clinical improvement.1

Chest CT showing multiple pulmonary nodules in the right lower lung field (red arrows).

Fungal hyphae are present on Gomori Methenamine-Silver (GMS) stain from CT-guided lung biopsy (x200).

CT of the neck revealed a mass-like lesion in the right lobe of the thyroid (green arrow).

Thyroid ultrasound reveals a 2.8×2.3 cm hypoechoic lesion in the right thyroid isthmus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fungal hyphae were present in the necrotic material from the thyroid abscess debridement (H&E, x400).
Learning points
Thyroiditis is a rare manifestation of disseminated fungal infection in immunocompromised hosts.
Aspergillus spp are the most commonly implicated pathogen, although there are reports of cases due to Cryptococcus neoformans, Histoplasma capsulatum, Coccidioides immitis and Candida spp.
Antifungal therapy targeting the culprit organism and consideration of surgical debridement are the mainstays of treatment.
Acknowledgments
Haresh Mani, MD Min Kim, MD.
Reference
Footnotes
Contributors CK, SK and AWB: planning, writing, revision. SC: planning, revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.