Article Text

Statistics from Altmetric.com
Description
A 50-year-old man with a history of iron-deficiency anaemia and fatty liver disease presented to the emergency department complaining of black tarry stools with associated weakness and shortness of breath for 1 week. At presentation, contrast-enhanced CT revealed multiple hypervascular masses in the abdomen and pelvis with the largest lesion located in the right lower quadrant, abutting the right psoas muscle (figure 1). Laboratory evaluation demonstrated a haemoglobin level of 5.5 g/dL (normal, 13.5–17.5 g/dL). Upper endoscopy showed a mass, which was making an extrinsic impression into the stomach (figure 2). Colonoscopy was unremarkable for abnormalities. Endoscopic ultrasound-guided fine-needle aspiration (FNA) of the lesion adjacent to the stomach was performed using a 22-gauge needle (Expect Slimline; Boston Scientific, Natick, Massachusetts, USA). The FNA was positive for metastatic carcinoma with hepatic features. Furthermore, capsule endoscopy identified blood clots surrounding the multiple, small intestinal masses. These lesions were subsequently identified as the metastatic hepatoid adenocarcinoma (HAC) based on the histopathological findings.

Contrast-enhanced CT abdomen and pelvis showing multiple peritoneal masses (coronal view).

Esophagogastroduodenoscopy showing extrinsic impression on the fundus of the stomach.
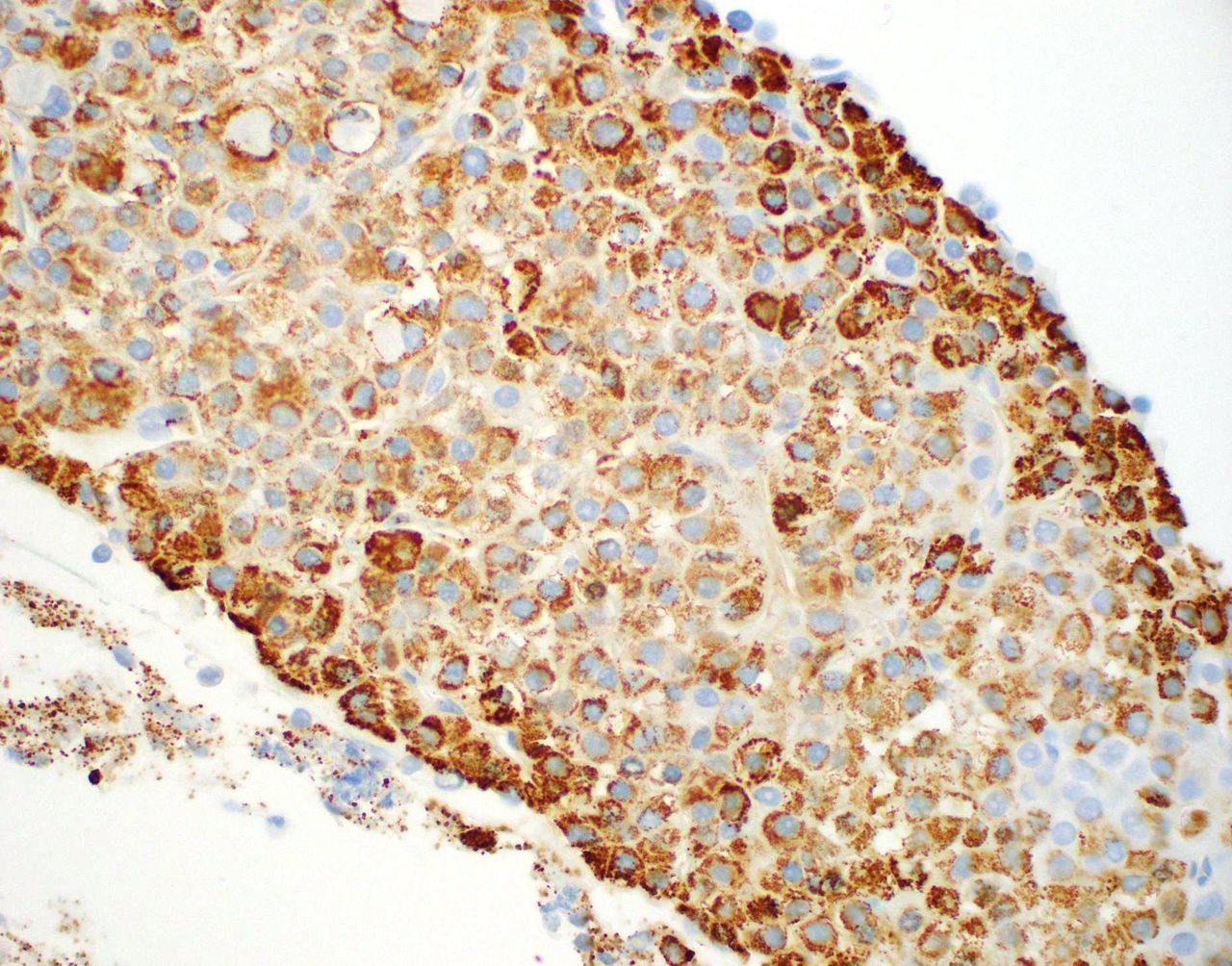
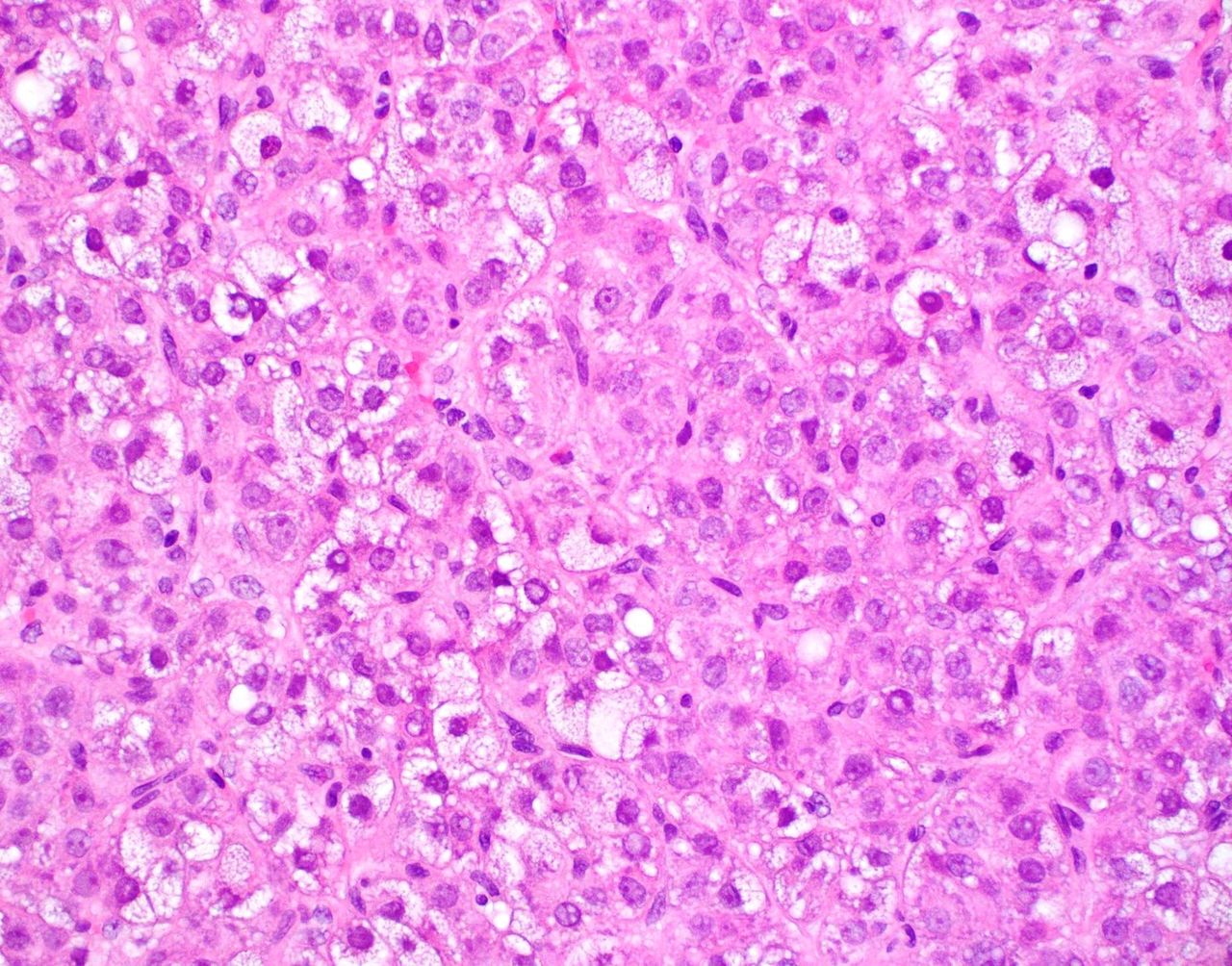
The patient then underwent exploratory laparotomy with biopsy to establish the aetiology of the peritoneal mass. The pathological examination of the biopsy specimen from the peritoneal mass in the right lower quadrant showed hepatoid cells with abundant eosinophilic cytoplasm (figure 3). The cells were positive for hepatocyte-specific antigen (figure 4). Additionally, hepatocellular markers, including glypican-3, arginase-1, alpha-fetoprotein (AFP), alpha-1 antitrypsin, carcinoembryonic antigen and cytokeratins 8/18 were also positive. His blood work revealed an AFP of 26 000 ng/mL (normal, <10 ng/mL). Biopsy was considered consistent with metastatic hepatocellular carcinoma, but there was no evidence of a primary liver lesion. Hence, the patient was diagnosed with primary peritoneal HAC. Unfortunately, the metastases were not amenable to surgical debulking; therefore, he was treated with 400 mg/day sorafenib (Nexavar, Bayer). A subsequent CT scan showed progression of the disease. Therein, he was switched to docetaxel (Taxotere, Sanofi) for palliation that demonstrated a relatively good response.

Pathological analysis of the peritoneal mass biopsy showing focal ballooned hepatoid cells having dense eosinophilic cytoplasm and large nuclei with minimal chronic inflammation (H&E staining; 200×).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Histology of peritoneal biopsy showing positive staining for hepatocyte-specific antigen (hepatocyte paraffin antigen-1 staining; 200×).
HAC is a rare neoplasm with close morphological resemblance to hepatocellular carcinoma, without tumour in the liver.1 Primary peritoneal HAC is an extremely rare clinicopathological entity. To the best of our knowledge, only seven cases in adults have been reported as of July 2018.2 Although the diagnosis of HAC is critical, clinicians frequently encounter difficulties in identifying these lesions. These tumours usually consist of large polygonal cells with abundant eosinophilic cytoplasm. While most hepatoid neoplasms express AFP, hepatocyte-specific antigen (hepatocyte paraffin-1) is considered to be more specific for hepatocellular differentiation.2 The data on the treatment of HAC are sparse, but existing literature confers a poor prognosis.3
It is notable that the gastrointestinal bleeding as an initial presentation of primary peritoneal HAC is unusually unique. In view of the potential risk of this neoplasm in patients with a new-onset gastrointestinal haemorrhage, as in the present case, gastrointestinal and/or peritoneal masses should be emergently investigated using appropriate immunohistochemical markers for an early diagnosis and treatment to limit morbidity and mortality. Therefore, it is important for clinicians to have a broad differential in these types of presentations given the clinical implications.
Learning points
Hepatoid adenocarcinoma (HAC) is a rare extrahepatic adenocarcinoma that morphologically and immunophenotypically mimics hepatocellular carcinoma. To our research, this is the eighth documented case of primary peritoneal HAC in the literature.
Differentiating primary peritoneal HAC from other tumours is a challenge and is also critical.
Due to rarity and heterogeneity of primary peritoneal HAC, no standard treatment exists.
The standard diagnostic and therapeutic algorithms are particularly warranted for these tumours, especially in patients with unusual initial presentations related to the gastrointestinal bleeding.
Acknowledgments
This case was presented as an abstract at the Annual Scientific Meeting of the American College of Gastroenterology, held on 13–18 October 2017 in Orlando, Florida, USA.
Footnotes
Contributors FI designed the study, performed the literature review, drafted the manuscript, reviewed the manuscript, revised the manuscript critically for important intellectual content and gave the final approval for the version published. FZ performed the literature review and drafted the manuscript. HTL reviewed the manuscript. WU contributed to the case presentation and suggested pertinent modifications.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.