Article Text

Statistics from Altmetric.com
Description
A 46-year-old man presented to us with lower urinary tract symptoms that include severe voiding symptoms. He had a history of injury to the perineum 3 years back. A smooth cystic swelling was palpable in the perineum in midline. Uroflowmetry was done and was suggestive of poor urinary flow (Qavg: 2 mL/s and Qmax: 6 mL/s), with significant postvoid residual urine (PVR). A micturating cystourethrogram (MCU) with retrograde urethrography (RUG) was done and was suggestive of an anterior urethral diverticulum, which was compressing the urethra, along with significant PVR (figure 1). The patient was planned for open excision of the urethral diverticulum. A cystourethroscopy was done preoperatively and clearly showed a normal anterior urethra and the opening of the diverticulum on the ventral aspect of the urethra (figure 2). The patient was operated in lithotomy position and a midline perineal incision was done. The diverticulum was dissected free and then excised, and the urethra was primarily closed over a 16F Foley catheter (figure 3). The catheter was removed after 2 weeks, after which the patient voided well. Six months postoperatively, the patient is doing fine.

Micturating cystourethrogram (MCU) and retrograde urethrography (RUG) of the patient demonstrating the anterior urethral diverticulum in the RUG and significant postvoid residual urine.

Cystourethroscopic view showing the opening of the diverticulum (arrow) and the normal urethra (arrowhead).

{kind=link}
{kind=link}
{kind=link}
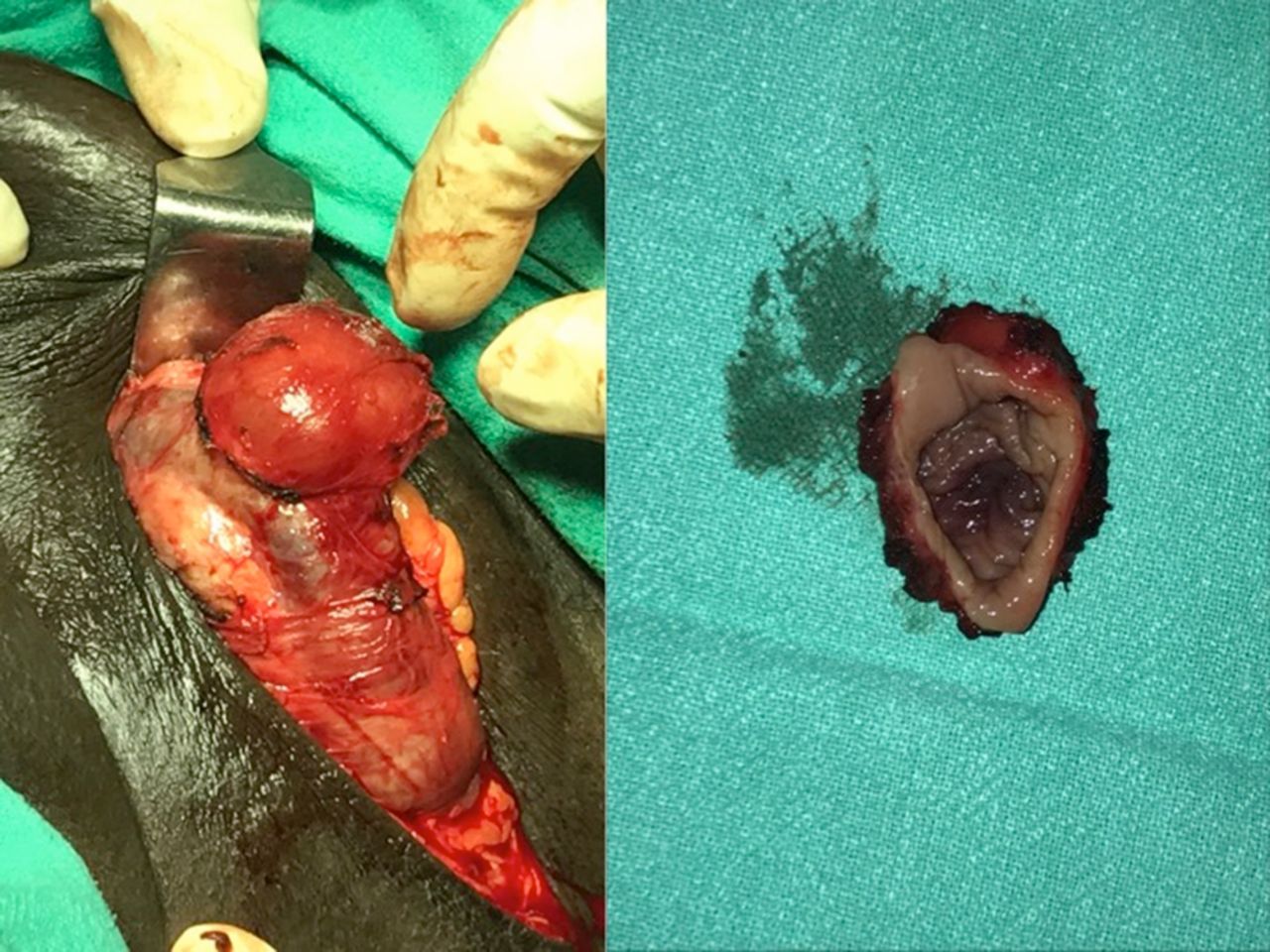
Intraoperative image of the diverticulum (left) and the excised diverticulum (right).
Anterior urethral diverticulum is a rare entity with description in the literature limited to case reports and a few small case series. Approximately two-thirds of cases of anterior urethral diverticulum are acquired, while the remaining one-third are congenital. Acquired urethral diverticulum can be secondary to trauma, stricture or previous surgery. Patients with urethral diverticulum may be asymptomatic or have voiding symptoms such as poor urinary stream, postvoid dribbling and urinary tract infection.1 It may be palpable clinically and may be compressible. A RUG with MCU may aid in the diagnosis of a urethral diverticulum. As in a female urethral diverticulum, MRI is not always required. Cystourethroscopy is a valuable tool in such cases as the opening of the diverticulum can be visualised easily.2 A small asymptomatic urethral diverticulum can be managed non-operatively by advising the patient to manually compress the diverticulum after voiding (so that there is no urinary stasis). Surgical options for management include endoscopic and open approaches. The endoscopic approach has a high chance of recurrence so an open approach is usually preferred. A small defect after excision of the diverticulum can be repaired by a primary longitudinal closure, whereas in larger defects a graft (eg, buccal) is required for urethroplasty.3
Learning points
Anterior urethral diverticulum in men is a rare condition, and its symptoms mimic other common conditions such as urethral stricture.
It may be clinically palpable, and retrograde urethrography and micturating cystourethrogram are useful in the investigation and diagnosis; cystourethroscopy is a valuable adjunct.
The best management for symptomatic urethral diverticulum is open excision, followed by primary closure of the urethra for short defects or placement of a graft for larger defects.
Footnotes
Contributors SP conceived the case report. SP and AA were major contributors towards the writing of the manuscript. AG, SP and DS treated the patient and also interpreted the patient data. SP and AA were involved in the review. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.