Article Text

Statistics from Altmetric.com
Description
The C-shaped root canal configuration is an anatomical variation of root fusion and a type of taurodontism commonly seen in the mandibular second molar with prevalence ranging from 2.7% to 45.5% in different populations.1 In this configuration, the root canals are connected by slit or web with varying anatomy along the root length which makes thorough debridement obstacle for the clinician.2 Cone-beam CT (CBCT) is a three-dimensional imaging technique that facilitates and improves understanding the complex morphology. This article presents a case of C-shaped root canal configuration of mandibular second molar managed by using CBCT and modification in obturation techniques.
A 40-year-old female patient reported with pain in the lower left back teeth region. Medical history of the patient was unremarkable. Intraoral examination revealed deep class I carious lesion on tooth 37 with tenderness on percussion. Thermal test was performed to check the vitality of the tooth which revealed dull pain, which was increased by heat and relieved by cold. Radiographically, deep dental caries was seen involving pulp without any periapical changes, there was radicular proximity of mesial and distal roots, a large distal canal and blurred image of a third canal in between. All the features were predictive of existence of C-shaped root canal (figure 1).3 The tooth was diagnosed with symptomatic irreversible pulpitis. Root canal treatment was planned and explained to the patient. Tooth was anaesthetised and isolated under rubber dam. Access cavity was prepared and visualised under surgical operating microscope (Carl Zeiss Surgical, Obenkochen, Germany). The floor of the pulp chamber showed three distinct orifices. The mesiobuccal and distal orifices were seen close together with a fin connecting two orifices, and the mesiolingual orifice was seen distance from the mesiobuccal and distal orifices which was similar to Min’s type III C-shaped root canal configuration (figure 2).4 The pulp chamber was irrigated with 5% sodium hypochlorite (Cmident India, Delhi). Working length was determined using apex locator (Root ZX II, J Morita, Tustin, California, USA) and confirmed with radiographs. In the radiograph, the K-file placed in the mesiobuccal canal was seen ending in distal foramen of the tooth (figure 3). Radiographically, the instrument is seen as if exiting the furcation and converging at the apex which is the most common feature of Fans C 2 Semicolon type C-shaped root canal configuration.5 CBCT (Carestream, Rochester, New York, USA) was taken to check the continuity of C-shaped root canal and rule out furcation involvement. Coronal third section revealed mesiobuccal and distal orifices close together connected by a fin and mesiolingual orifice seen existing separately at a distance. Middle third section revealed radicular lingual groove suggestive of incomplete fusion between two roots resulting in C-shaped root canal and three separate orifices.5 Apical third section revealed mesiobuccal and distal root canals joining to form one single C-shaped root canal from middle third to apical third of the root (figure 4). Cleaning and shaping were completed using K files (Mani, Japan) with circumferential anticurvature filing and self-adjusting rotary files (SAF, Redent Nova, Israel). Ultrasonic activation of irrigant enhanced necrotic tissue removal. In the next appointment, master cone radiograph was taken which confirmed the apical extension of gutta percha. Thermoplasticised gutta percha technique and warm vertical condensation are the recommended techniques for C-shaped root canals. The case treated presents Fan’s radiographic type III,5 since case reports with such type of root canal configuration used lateral condensation technique, we used the same technique and found good results with gutta percha and AH Plus (Dentsply Maillefer Company, USA) as endodontic sealer into the complex anatomy of the root canal (figure 5).6 7

Preoperative radiograph showing conical fused roots.

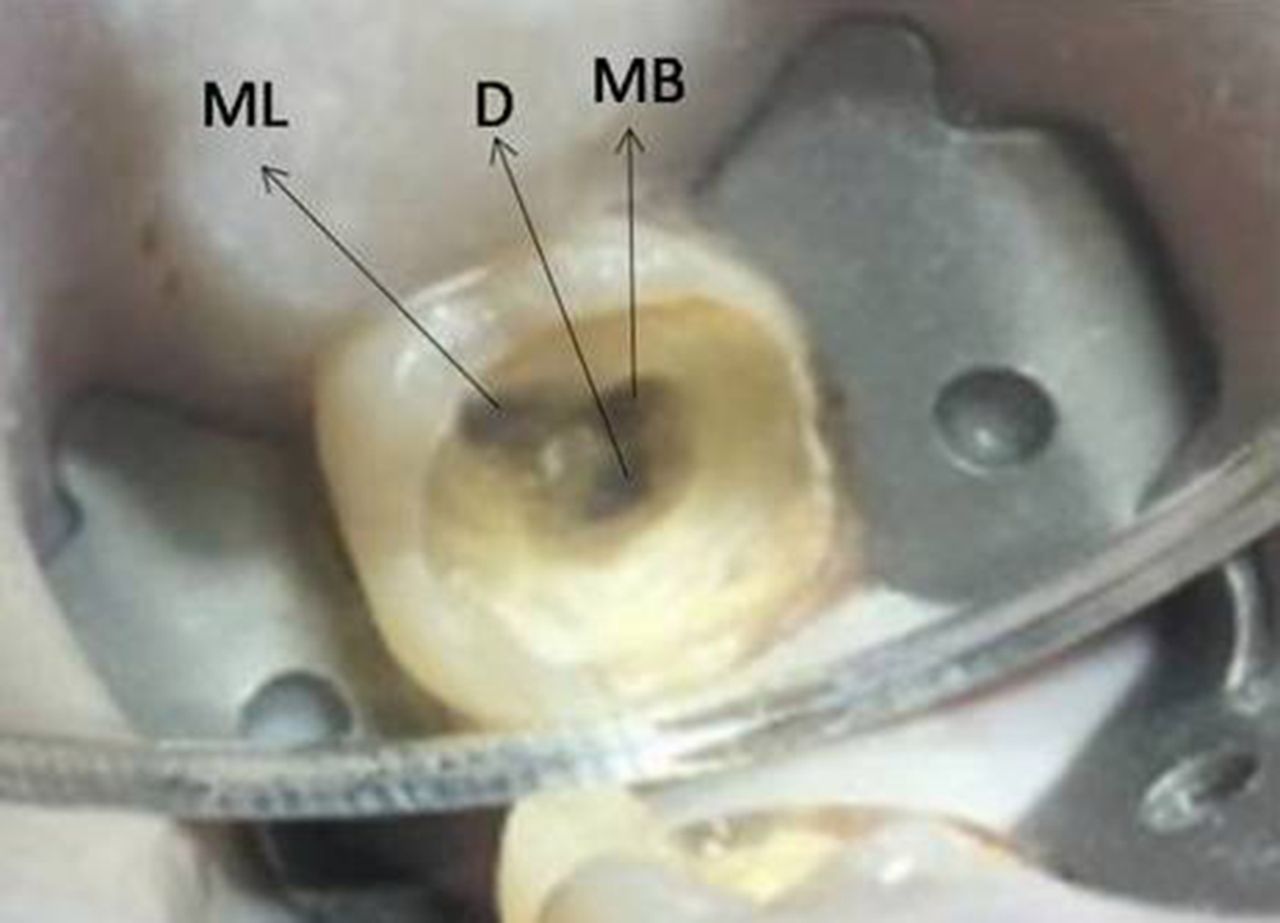
Access cavity preparation showing three distinct orifices. D, distal; MB, mesiobuccal; ML, mesiolingual.

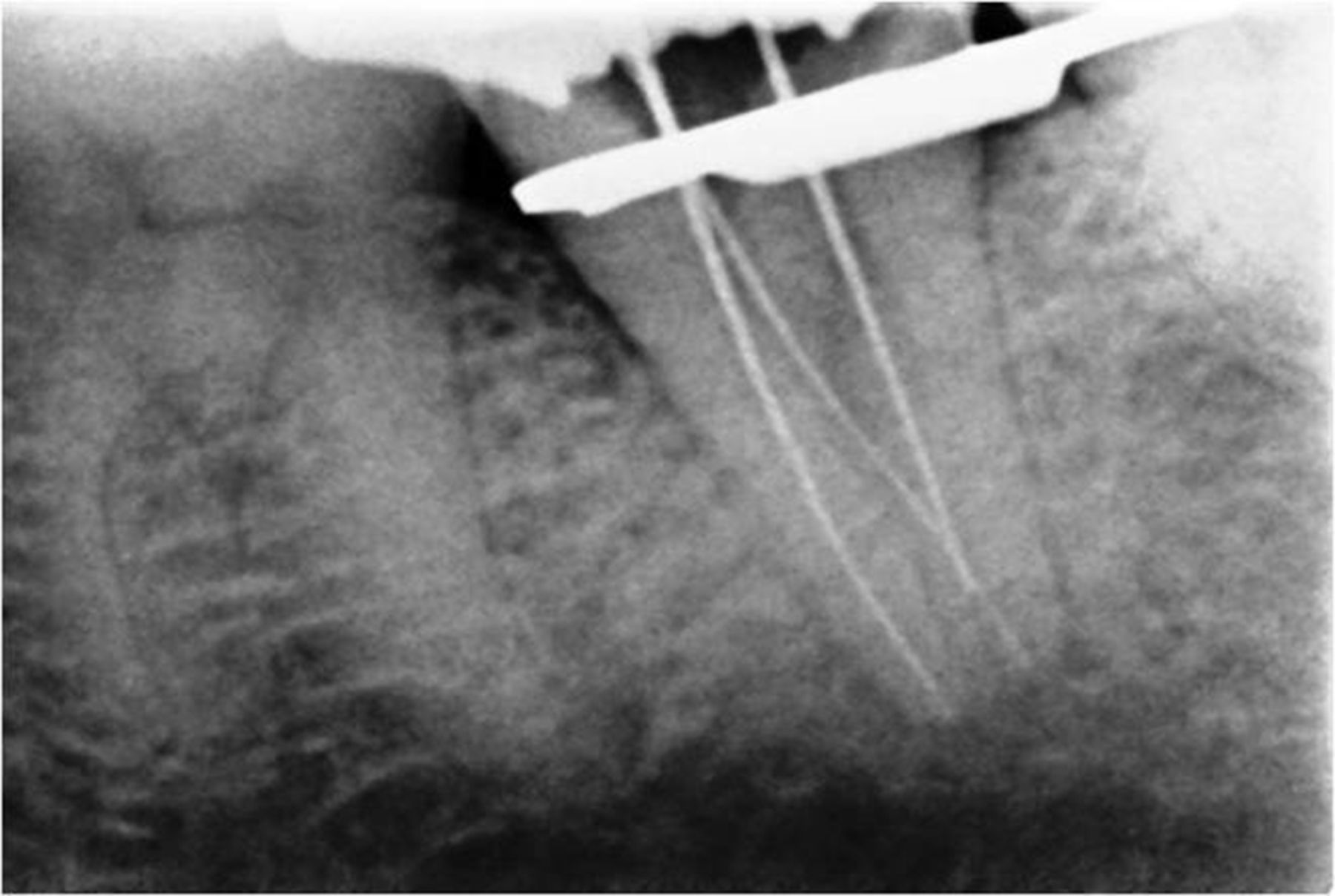
Working length determination showing mesiobuccal root canal ending in distal foramen.
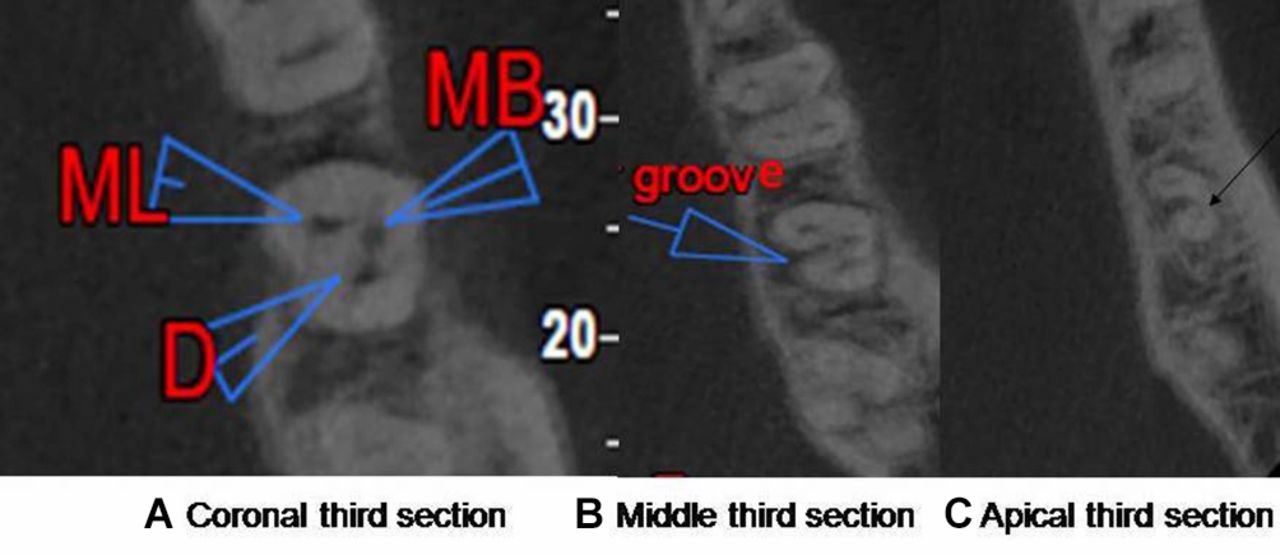
Cone-beam CT axial images: (A) Coronal third section showing mesiobuccal (MB) and distal (D) orifices close together connected by a fin and mesiolingual (ML) orifice seen existing as a separate canal. (B) Middle third section showing radicular lingual groove suggestive of incomplete fusion between two roots. (C) Apical third section showing MB and D root canals joining to form one single C-shaped root canal from middle third to apical third of the root.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
One-month postoperative radiograph.
Learning points
Usage of diagnostic aids like cone-beam CT and operating microscopes help in understanding the anatomical variations.
Continuous circumferential anticurvature filing along the periphery of the C-shaped root canal assisted with ultrasonic activation of sodium hypochlorite enhances tissue removal.
Modifications in obturation techniques like lateral and warm vertical condensation help in increasing the adaptation and density of filling.
Footnotes
Contributors AL has done the case. DKS and SS have prepared the manuscript. NS has taken the photographs.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.