Article Text

Statistics from Altmetric.com
Description
A 78-year-old woman with history of Addison’s disease, hypothyroidism, hypertension and recent hospital admission for asthma exacerbation requiring hospitalisation for steroid pulse presented to the emergency department with 1 day of significant epigastric and right lower quadrant pain. Her pain steadily worsened and was associated with nausea and clear emesis. She was on a steroid taper for her recent asthma exacerbation, and she is normally on baseline low-dose steroids for her Addison’s disease.
On evaluation in the emergency department, the patient was noted to be tachycardic in the 100s but otherwise haemodynamically stable. Her abdomen was distended, and she endorsed moderate to severe tenderness over her right lower quadrant with guarding but no rebound. Her labs were notable for white cell count of 31.6x109/L and a lactate of 4.5 mmol/L.
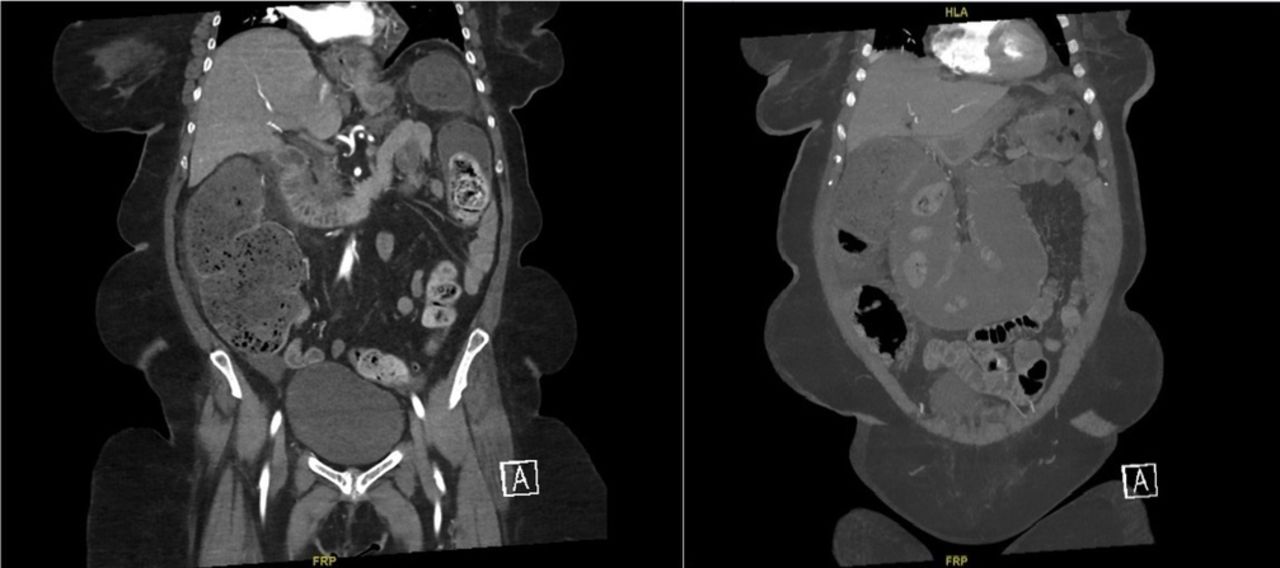
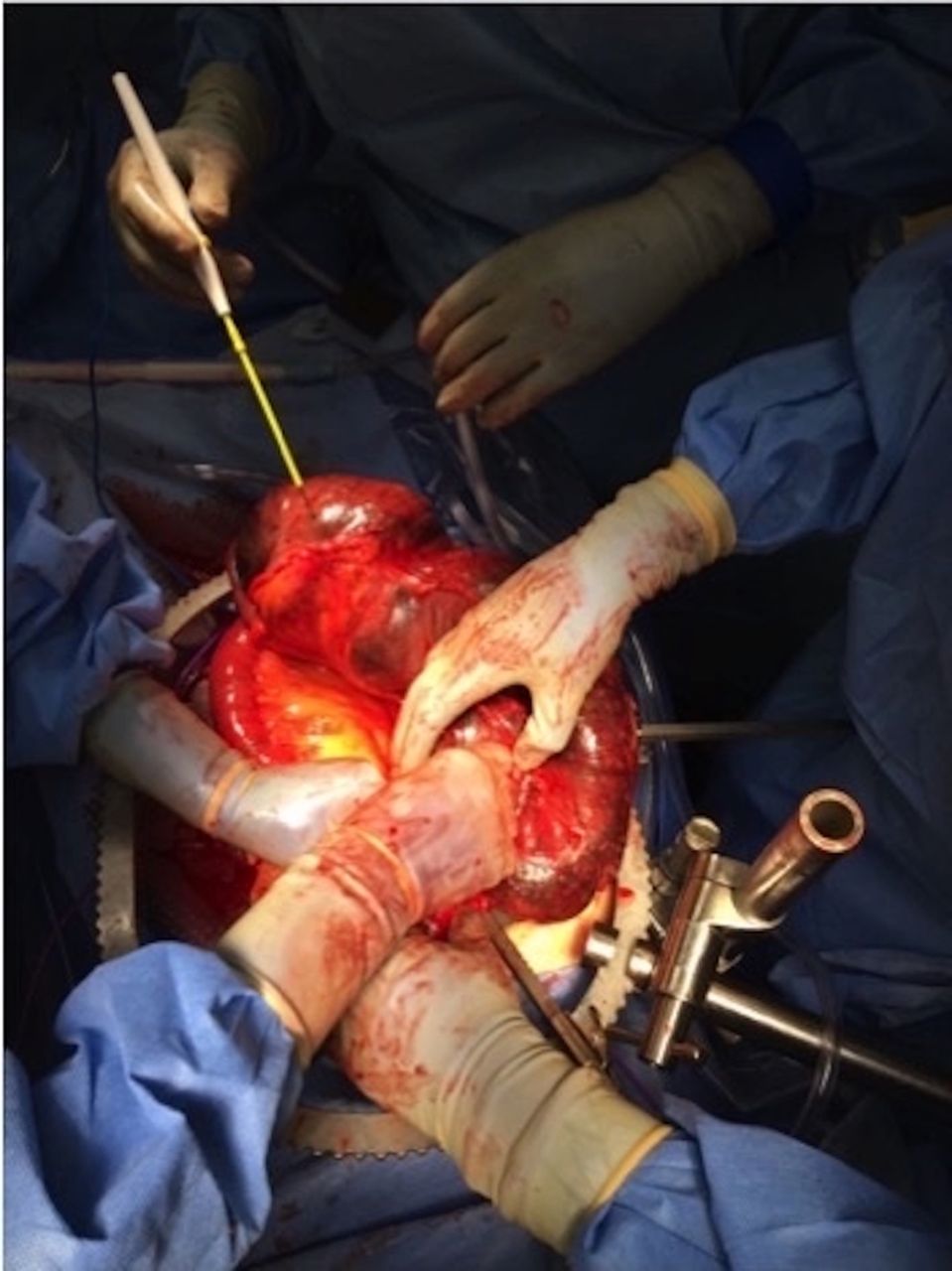
The patient was promptly fluid resuscitated, given intravenous antibiotics and analgesics. Given concern for bowel ischaemia, an abdominopelvic CT angiogram was obtained and revealed a 4.1 cm fecalith in the mid-descending colon causing significant dilation of transverse and ascending colon, with caecal dilation to 8.3 cm (figure 1). No pneumatosis, bowel wall thickening or inflammation was appreciated to suggest bowel ischaemia. Gastroenterology was asked to assess the patient for endoscopic fecalith removal, but the patient’s blood pressures decreased to systolics of 90s from 130s with persistent tachycardia and worsening abdominal pain. Endoscopy was deferred and she was taken urgently to the operating room for exploratory laparotomy. On entry of her abdomen, it was apparent that her entire colon proximal to the fecalith was frankly necrotic (figure 2). There was no overt perforation, but there was murky fluid appreciated throughout abdomen. A subtotal colectomy with end ileostomy was performed. Her abdomen was copiously irrigated and her incisions were closed primarily.

The left image displays a 4.1 cm obstructing fecalith in descending colon with clear transition point and significantly dilated caecum. There was no evidence of bowel wall thickening, fat stranding and perforation to suggest vascular compromise. Significantly dilated transverse colon seen in the right image.

{kind=link}
{kind=link}
Intraoperatively, colon was frankly necrotic and foul smelling. There was murky fluid throughout abdomen, but no feculence or perforation was appreciated. A rock-hard fecalith was appreciated at the mid-descending colon and was mobile within the lumen.
She was admitted to the intensive care unit postoperatively and recovered well. She was extubated and weaned off all vasopressors on postoperative day 1 and her ileostomy was functioning by postoperative day 5. She was discharged to a rehabilitation facility 2 weeks after her surgery.
Learning points
Fecaliths are generally considered a benign condition that can often be resolved with non-surgical interventions, including mineral oil enemas, manual disimpaction and polyethylene glycol (either orally or through a nasogastric tube). If these interventions fail, endoscopic fragmentation of the fecalith may be necessary.
Rarely, fecaliths can lead to more serious complications. Obstructive uropathy and stercoraceous ulcers are generally resolved with endoscopic removal of the obstructing fecalith. However, persistent intestinal obstruction leading to bowel wall compromise or perforation is a surgical emergency.
This case illustrates a rare but life-threatening complication of fecalith. The patient developed a necrotic colon and was symptomatic over just a 24-hour period. Moreover, fecalith complications are usually present in patients who are institutionalised or have neurologic disorders (eg, paraplegics). Our patient was an overall healthy woman who was living independently, suggesting that complications are not restricted to specific patient populations.
Footnotes
Contributors Conception or design of the work: DM, MV, NM. Data collection: DM, MV, NM. Data analysis and interpretation: DM, RA, MV, NM. Drafting the article: DM, RA. Critical revision of the article: DM, RA, MV, NM. Final approval of the version to be published: DM, RA, MV, NM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.