Article Text

Statistics from Altmetric.com
Description
A previously healthy 28-year-old woman presented with generalised maculopapular lesions (figure 1) since 10 days which were associated with low-grade, intermittent fever. Six days following this, she developed double vision and swaying while walking. There was no history of headache, vomiting, seizure or limb weakness. There was no significant medical history and neither she was on any drug therapy. On examination, she had generalised maculopapular rashes typical of varicella zoster virus (VZV) infection. There was internuclear ophthalmoplegia (figure 2) with bilateral vertical nystagmus on upgaze. Other cranial nerves, and motor and sensory system examinations were normal. Cerebellar function tests like finger-nose test on right side and tandem walking test were impaired. Patient tends to sway on either side while walking. The cardiovascular and respiratory system examinations were normal.

Generalised maculopapular rashes.

Left medial rectus palsy.
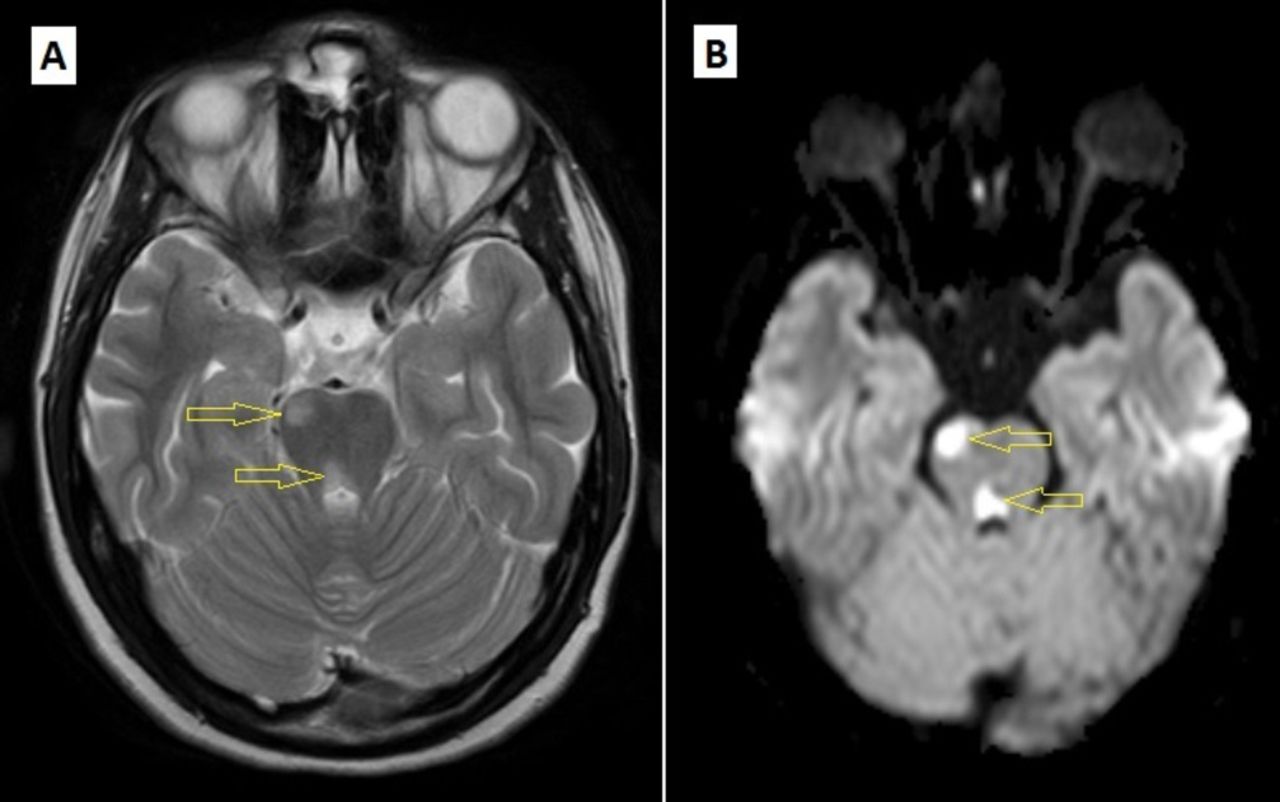
Initial laboratory investigations like complete haemogram, and renal and liver function tests were normal. MRI brain revealed an acute infarct in the right hemipons and superior cerebellar peduncle (figure 3) which could explain her neurological deficits. A complete diagnostic workup was conducted to identify the underlying cause of the stroke, which included cardiac echocardiography, bilateral carotid-vertebral Doppler, MRI angiography of cerebral vessels, antinuclear antibodies, antineutrophil cytoplasmic antibodies, antiphospholipid antibodies and HIV ELISA which were all negative. Lumbar puncture revealed normal pressure with no abnormalities in cerebrospinal fluid (CSF) studies. PCR for VZV was positive.
{kind=link}
{kind=link}
{kind=link}
MRI brain. (A) T2 weighted and (B) diffusion weighted showing acute infarcts in right hemipons extending up to right superior cerebellar peduncle.
The patient was started on intravenous acyclovir, antiplatelet and other supportive therapy following which there was progressive improvement in her symptoms.
VZV infection is characterised by presence of generalised maculopapular rashes and fever. Presenting as a milder form in children, the disease is generally more severe in adults and can have a wide array of complications. The virus present within the skin lesions has been found to migrate along the sensory nerve axons in a centripetal manner towards the regional nerve ganglion. In most cases, the virus becomes latent within the ganglion and often gets reactivated at an older age, resulting in herpes zoster.1 However, in few immunocompromised patients, the infection could spread rapidly resulting in migration of the virus to the central nervous system from where it can enter the cerebral vessels, infecting the endothelial lining of the artery leading to vasculopathy. Middle cerebral artery is found to be most commonly involved.2 Interestingly, our patient had posterior circulation stroke and she is immunocompetent; both findings were unusual.
The diagnosis can be established by testing of VZV antibody and VZV PCR in the CSF, and exclusion of all other possible causes of stroke. Immunocompromised states may be coexisting and hence must be tested for HIV. Because VZV vasculopathy is uncommon, there are no controlled treatment trials to assess the optimal treatment strategies. Patients are typically treated for a minimum of 14 days with acyclovir intravenously based on the clinical experience of experts and descriptive case series. The value of antiviral therapy to prevent stroke is less clear.3 With timely intervention, the condition is reversible and the patient can recover with no long-term sequelae.
Learning points
Varicella zoster virus (VZV) infection in adults could result in complications such as pneumonia and encephalitis, but presenting as stroke is very rare.
Patients may present with acute or subacute infarction and commonly involves vessel being middle cerebral artery. Involvement of posterior circulation is very rare.
The incidence of VZV vasculopathy is higher in immunocompromised individuals but may also occur in immunocompetent patients.
A high index of clinical suspicion, efforts towards early diagnosis and initiation of acyclovir therapy are required to prevent complications.
Acknowledgments
The authors thank the Department of Radio Diagnosis for providing MRI pictures and all the colleagues who were involved in the patient care.
Footnotes
Contributors SPM and NG wrote the draft of the manuscript. AS provided the clinical pictures. RVA was involved in patient management and revised the manuscript critically for important intellectual content. All authors contributed to the literature review and approved the final manuscript for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.