Article Text

Statistics from Altmetric.com
Description
A 49-year-old non-diabetic woman was admitted to our hospital with complaints of fever of unknown origin (FUO) of 2 months’ duration. The patient has no recent history of exposure to tuberculosis (TB). Systemic examination revealed pallor and tender splenomegaly. Blood investigations revealed a microcytic hypochromic anaemia with haemoglobin of 7.5 g/dL, total leucocyte count of 12.7x10∧9/L and a raised erythrocyte sedimentation rate (ESR) (62 mm/hour). The rest of the FUO work-up, including blood cultures, serologies, chest radiograph, Mantoux and echocardiography, was unremarkable. Contrast-enhanced CT of the abdomen revealed multiple splenic abscesses (figure 1), from which a diagnostic and therapeutic single time aspiration was done. Around 10 mL of pus was aspirated which showed smear positivity for Mycobacterium tuberculosis (figure 2). The patient was subsequently started on four-drug antitubercular treatment. The fever subsided and repeat serial ultrasound imaging showed resolution of splenic abscess. Primary splenic TB in an immunocompetent patient is a rare entity but should be considered as a diagnostic possibility especially in a country where TB is endemic.

CT scan of the abdomen showing multiple conglomerating hypodense lesions in the splenic parenchyma suggestive of abscesses.

{kind=link}
{kind=link}
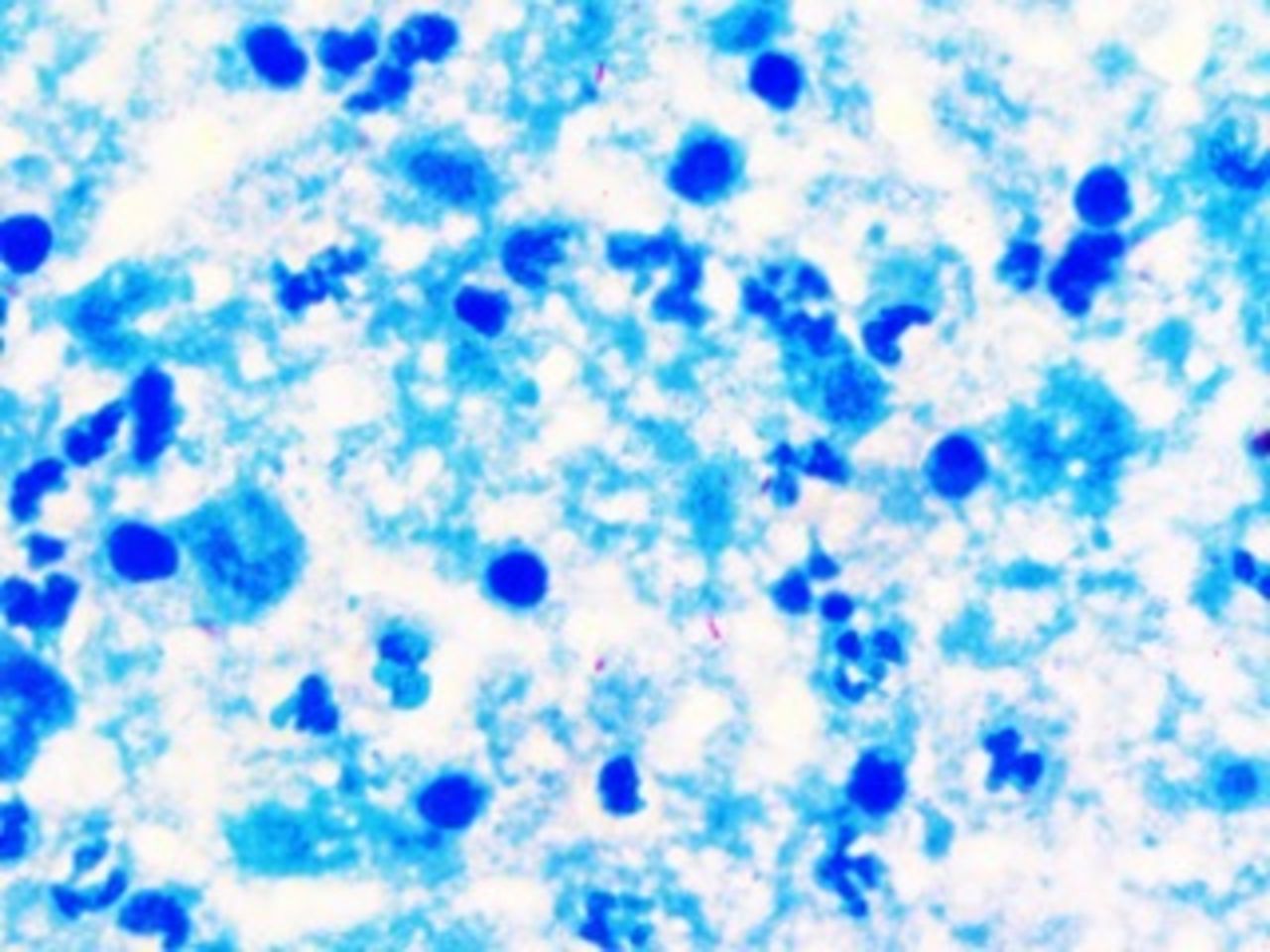
Smear from pus aspirated from splenic abscess showing degenerated neutrophils, macrophages in a background of necrosis and stained positive for acid-fast bacilli.
Splenic abscess has a very low incidence (0.1%–0.7% on autopsy) and tubercular splenic abscess is even rarer.1 Usually spleen is involved in disseminated TB, and primary splenic TB is extremely uncommon with only few cases published in the literature.1–4 Splenic abscess is mostly seen in patients with underlying immunocompromised state, which includes diabetes, transplant recipients, intravenous drug abuse and retropositivity.1 It is most commonly caused by Gram-negative organisms, with Klebsiella as the most commonly isolated organism.5 CT differentials of the splenic abscess include splenic lymphoma, metastasis, parasitic cyst, infarction, haemangioma, sarcoidosis and trauma. Differentiating tubercular from pyogenic splenic abscess on CT can sometimes be difficult; however, unilocular abscess, rim enhancement and gas formation within the lesion favour pyogenic abscess.6 Treatment consists of antitubercular therapy and spleen-saving surgery such as percutaneous single time aspiration.5 The above case is presented because of the rarity of occurrence of primary splenic TB and its successful management with single time splenic aspiration and antitubercular drugs.
Learning points
Splenic tuberculosis should be considered in patients with fever of unknown origin and splenomegaly especially in our country where tuberculosis is endemic.
Ultrasonography of the abdomen can be a useful and cost-effective mode to suspect this rare entity.
Footnotes
Contributors JS and AS: writing, concept, image acquisition. KLG: proof-reading, corrections.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.