Article Text

Statistics from Altmetric.com
Background
Aspergillosis comprises a spectrum of diseases related to host factors.1–3 Invasive aspergillosis (IA) is a disease of concern due to high mortality in transplant recipients and patients with haematological malignancies. Although rare, its occurrence has been reported in immunocompetent hosts, with multisystem involvement.4–6 Here, we present a case of a young immunocompetent man presenting with signs of superior vena cava (SVC) obstruction and a mediastinal mass. Suspicion of a malignancy was high but on biopsy was found to have IA of the mediastinum.
Case presentation
A 28-year-old man was referred to our pulmonary outpatient clinic (Aga Khan University Hospital, Karachi) for the workup of a mediastinal mass. He had a 12-month history of right-sided chest pain, with radiation to the back. He also complained of shortness of breath, reduced appetite, weight loss, difficulty swallowing and swelling of his face and neck for the past 5 months. He denied fever, night sweats, cough or past tuberculosis (TB) contact. He had a history of smoking in the distant past, that is, 2 years of smoking around 10 years ago. He denied alcohol and illicit drug use. He sought medical attention 6 months after his symptoms began in his hometown. He was started on treatment for asthma, that is, inhaled corticosteroids and inhaled long-acting beta-agonist and a 3-week tapering dose of oral prednisolone (starting at 10 mg twice a day) with no improvement whatsoever. A chest X-ray (CXR) was ordered and a suspicious finding on that led to a CT of the thorax, which showed a mediastinal mass. Despite two negative sputum samples for acid-fast bacilli (AFB), he was started on empiric antituberculous therapy. This was discontinued after 3 weeks as there was no clinical improvement.
He was then referred to us for further workup and management with a strong suspicion of malignancy (likely lymphoma).
On initial assessment, vital signs were within normal values. There was evidence of congested neck, prominent chest wall veins and facial plethora (figure 1).

Right anterior neck and chest wall showing prominent neck and chest wall veins and mediastinotomy scar.
Chest examination revealed absent breath sounds on the lower one-third of the right posterior chest and an otherwise unremarkable cardiovascular and systemic examination.
Investigations
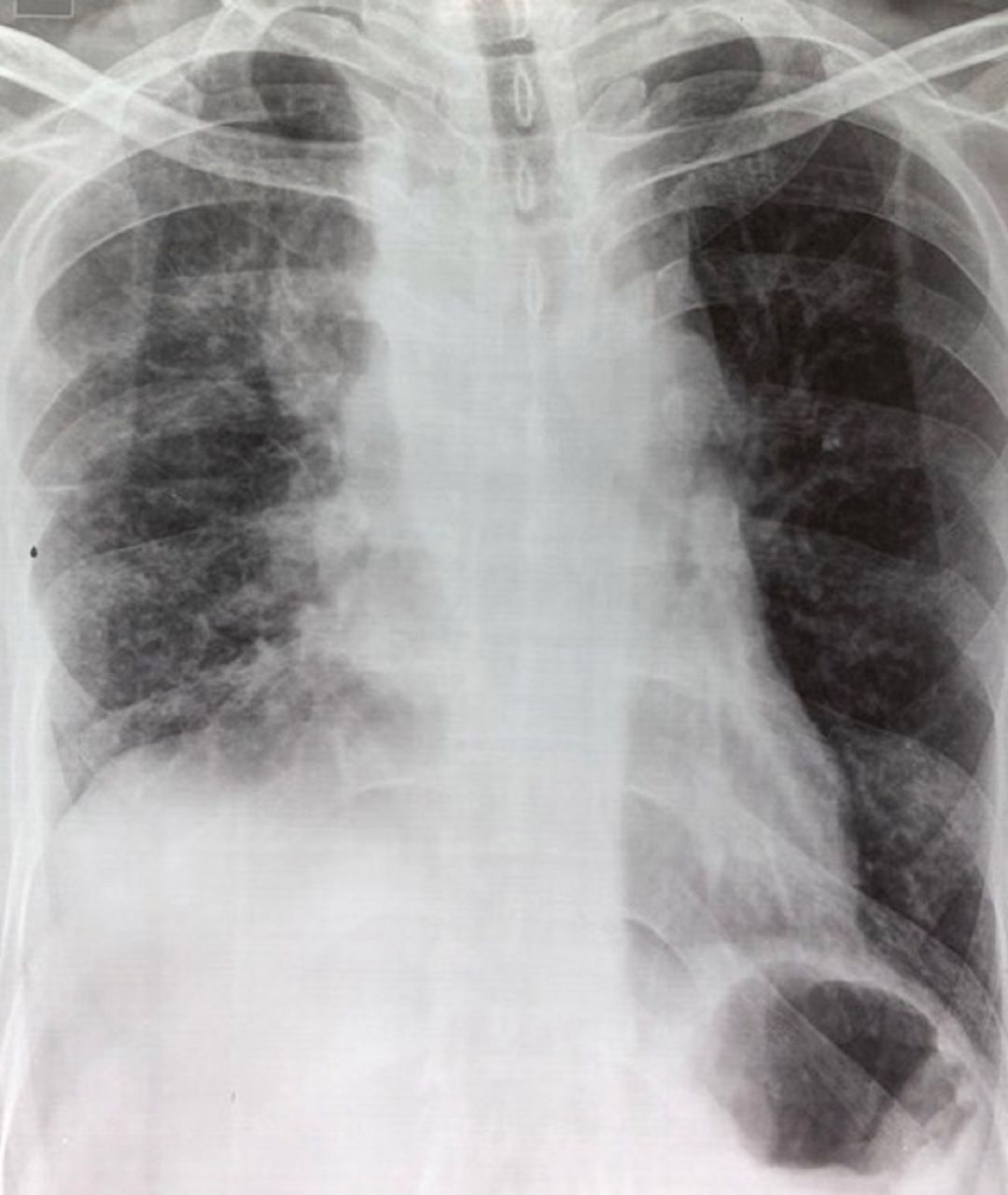
Laboratory tests were normal. CXR was concerning for a widened mediastinum and right-sided effusion (figure 2).
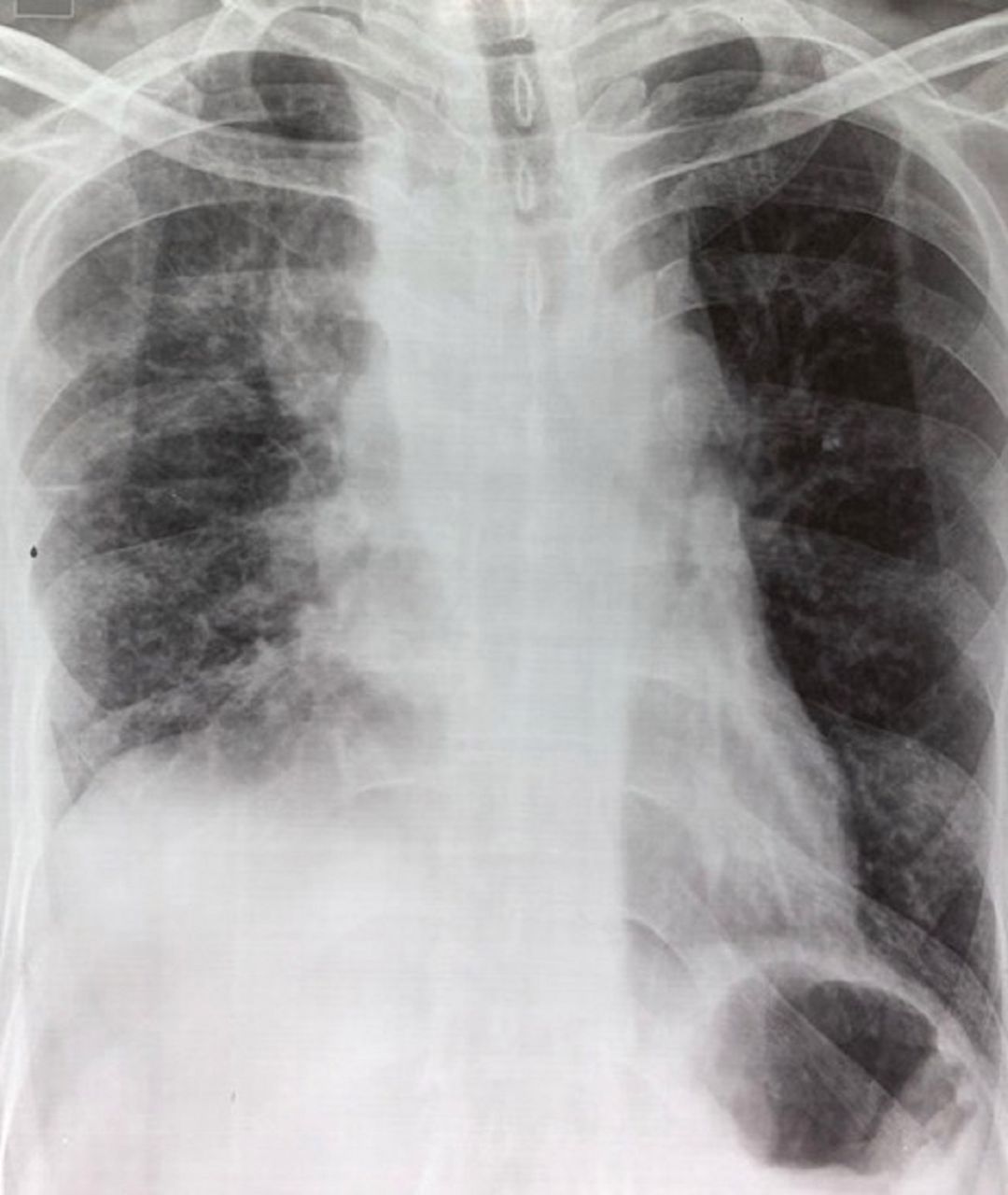
Chest X-ray showing widened mediastinum, elevated right hemidiaphragm and blunting of the right costophrenic angle.
Diagnostic thoracentesis revealed a lymphocyte dominant exudate, a white cell count of 6.673×109/L (lymphocytes 95%), protein of 4.8 g/dL, glucose of 88 mg/dL and Lactate dehydrogenase (LDH) of 323 U/L. Pleural fluid cytology revealed no malignant cells. Serological testing for HIV was negative. Serum immunoglobulin (IgG, IgA, IgM) levels were within normal range.
CT thorax showed an 11×9×8 cm mass centred in the anterior and middle mediastinum, more on the right side. It showed invasion of the right atrium, right pulmonary artery with partial invasion of the left atrium and left inferior pulmonary vein. Partial obliteration of the right main stem bronchus was noted along with narrowing of the SVC and prominent collaterals (figure 3A–C).
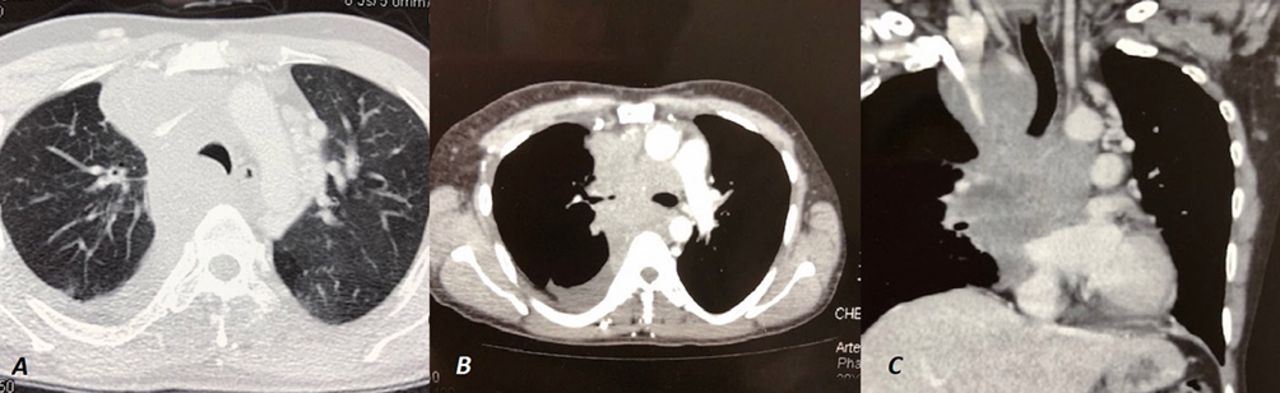
CT of the chest. (A) Lung window showing right anterior mediastinal mass with right-sided effusion. (B) Mediastinal window showing mediastinal mass occluding right main bronchus. (C) Coronal section showing invasion of the mediastinal structures.
Outcome and follow-up
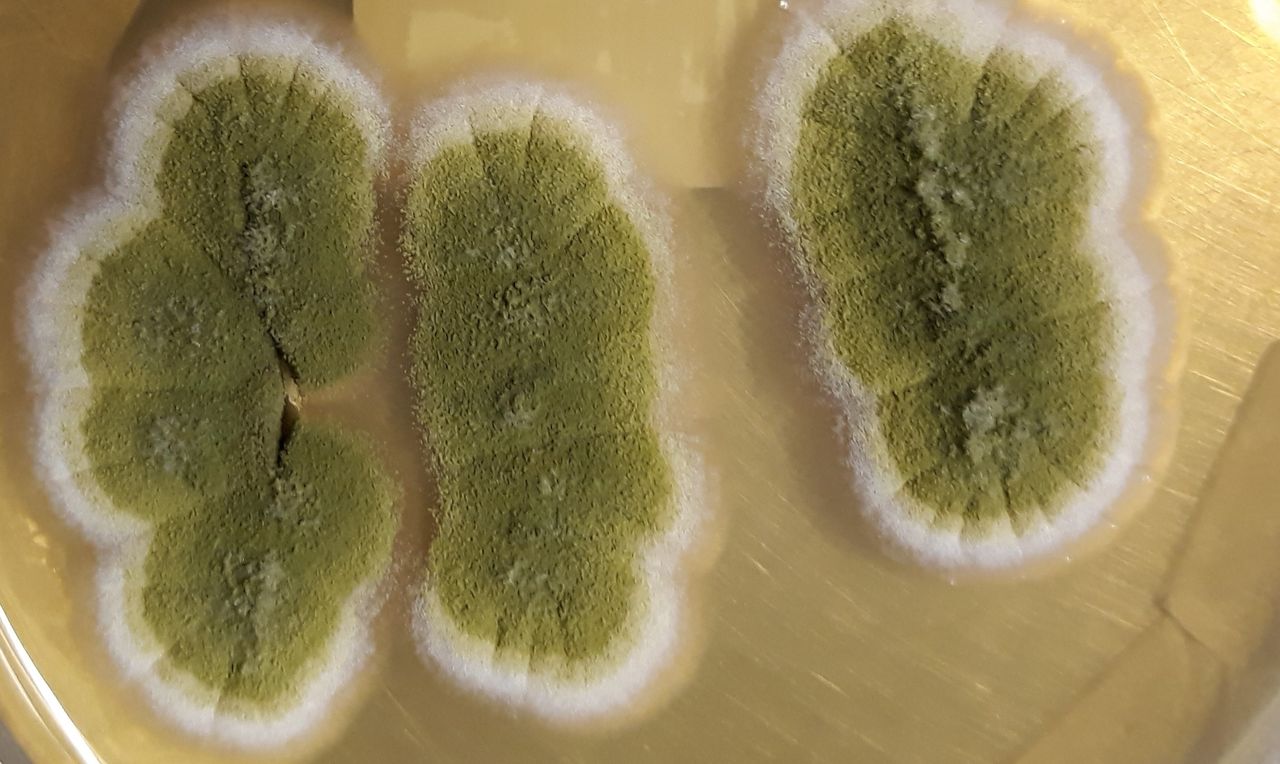
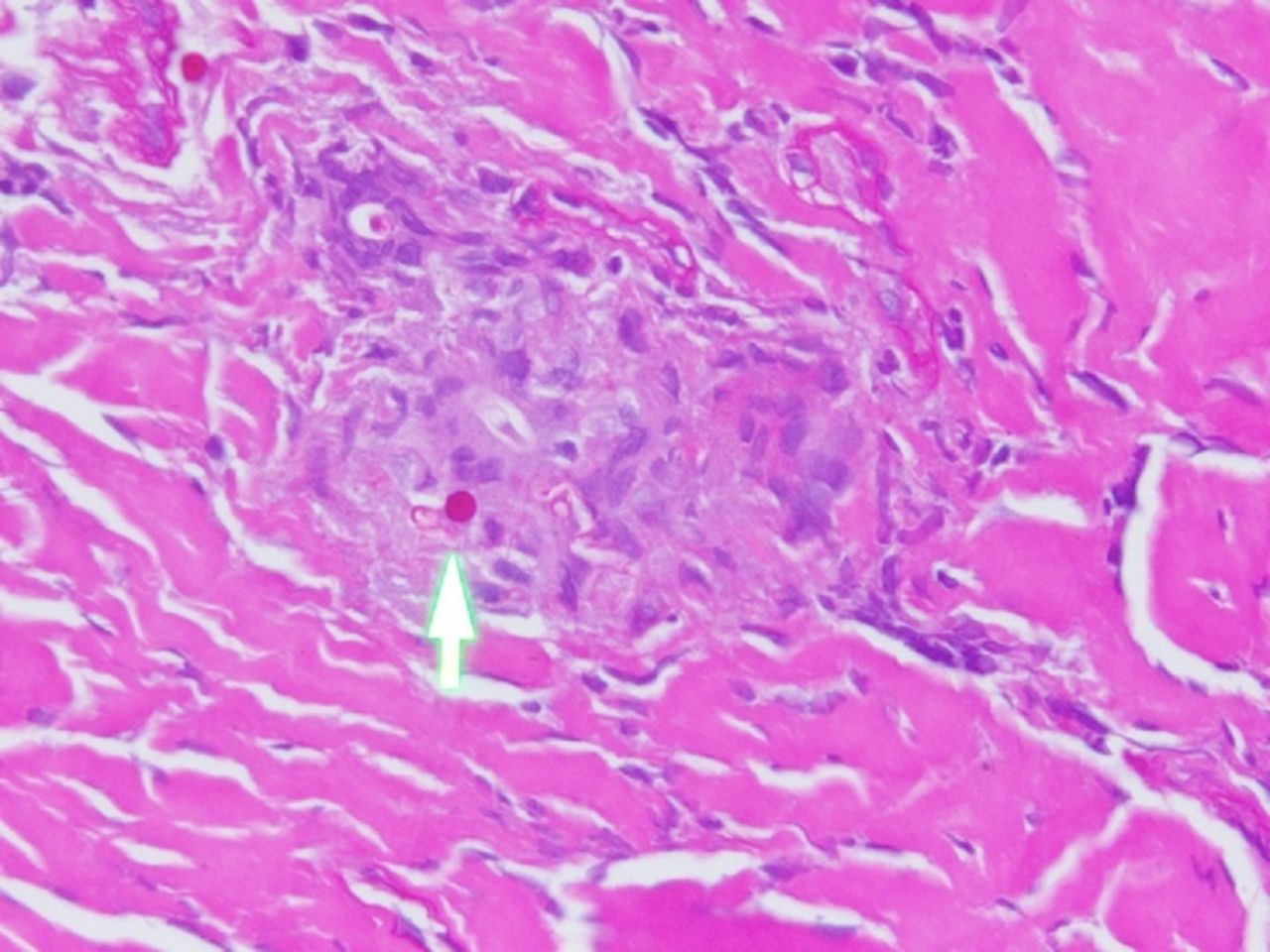
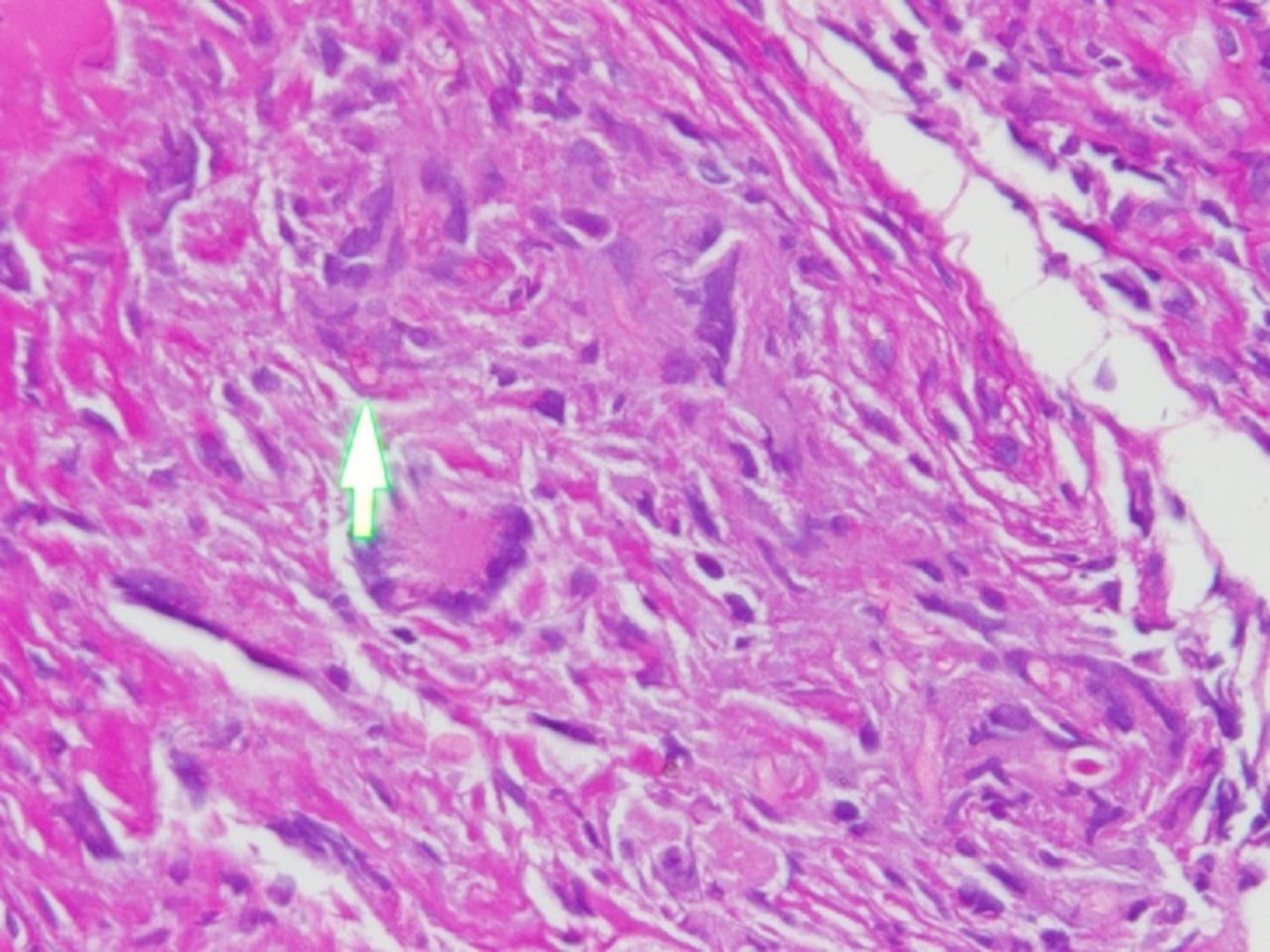
He underwent anterior mediastinotomy, with mediastinal mass biopsy, revealing non-necrotising granulomas, with multinucleated giant cells and histiocytes. Scant fragments of fibrocollagenous tissue noted. Periodic acid-Schiff and Gomori methenamine-silver stains highlighted occasional septate fungal hyphae (figures 4, 5 and 6). Mycology cultures grew the Aspergillus flavus complex (figure 7). Mediastinal tissue AFB smear and culture were negative.

Periodic acid-Schiff stain highlighting mostly fungal spores, rare hyphae seen.
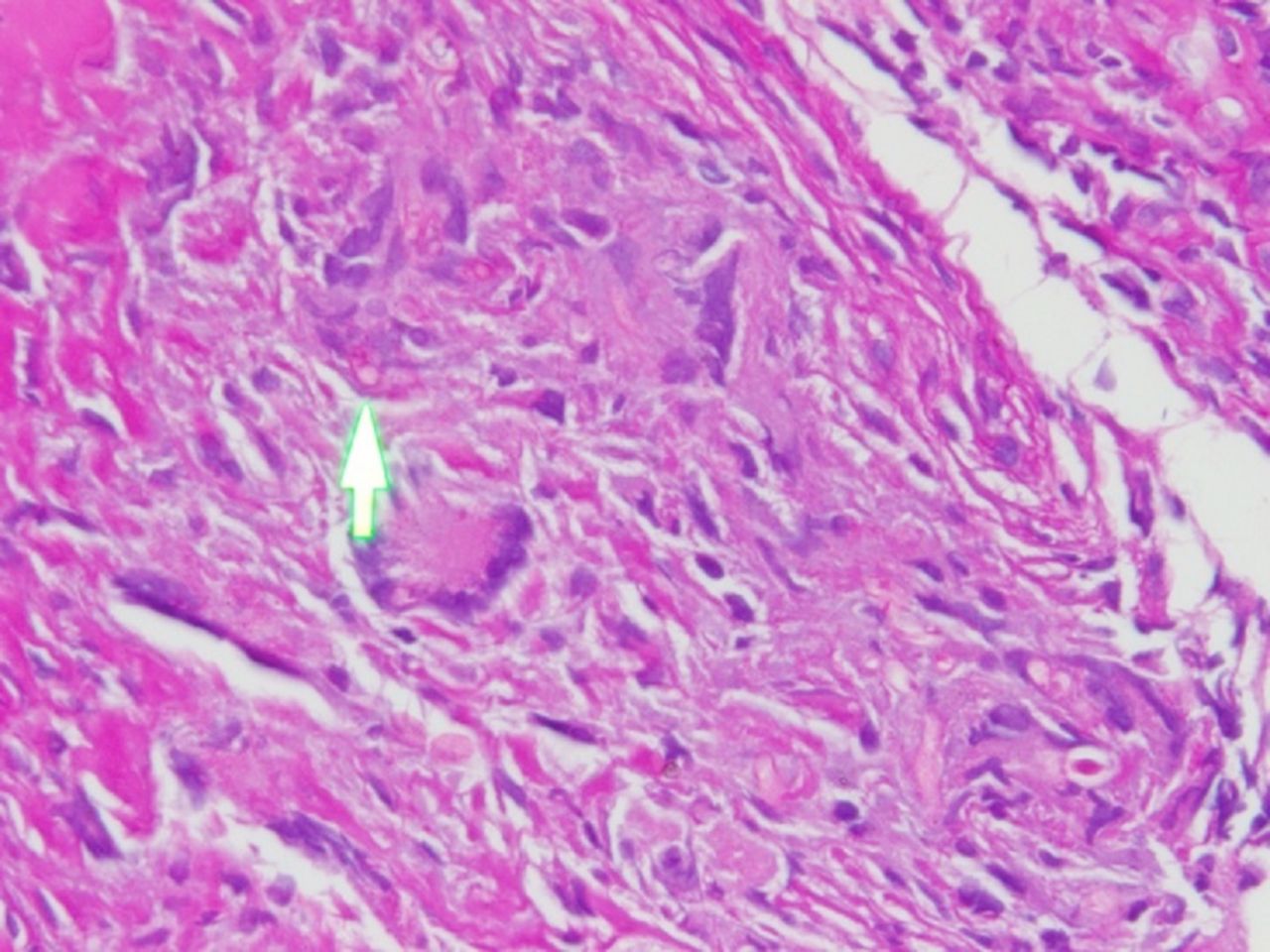
Periodic acid-Schiff stain highlighting mostly fungal spores, rare hyphae seen.

Gomori methenamine-silver stain, highlighting fungal bodies.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Aspergillus colonies.
Therapy with oral voriconazole 400 mg twice a day for 1 day followed by 200 mg twice a day was started after histological confirmation, and the patient was asked to follow up in 4 and then 8 weeks, while continuing therapy. Patient showed marked improvements in symptoms with progressive weight gain and increased oral intake. Repeat CT scan is planned at 6 months to look for mass resolution.
Discussion
To the best of our knowledge, this is the second case of SVC obstruction secondary to IA of the mediastinum in an immunocompetent host published in the literature. Association with other infectious diseases namely syphilis, TB, histoplasmosis and actinomycosis have been described.
Aspergillus is a spore-forming saprophytic fungus, ubiquitous to the environment. With approximately 200 species, Aspergillus fumigatus is the most commonly isolated pathogen.
Aspergillus species cause a broad spectrum of disease, ranging from hypersensitivity reactions to direct angioinvasion. The lung is the most common site of infection with disease ranging from allergic bronchopulmonary aspergillosis, chronic necrotising pneumonia, aspergilloma and IA.6
IA is primarily a disease of immunocompromised patients, with prolonged neutropenia constituting a predominant risk factor,7 followed by haematopoietic stem cell transplants or solid organ transplants (especially lung transplantation) and advanced AIDS.8 9 In the above population of patients, host factors govern the risk and clinicopathological features of invasive disease.1 2 Rarely invasive pulmonary aspergillosis may complicate chronic obstructive pulmonary disease, particularly when treated with oral corticosteroids (OCS), bacterial or viral pneumonia, sepsis, liver failure, alcoholism or sinusitis.10–12
Our patient’s laboratory findings revealed no evidence of neutropenia or immunosuppression, raising a suspicion of whether his 2-year smoking history or 3-week history of OCS use could have led to some abnormalities in the pulmonary defence mechanism. This seemed an unlikely possibility as the patient was symptomatic months before inhaled or OCS therapy was prescribed.
The respiratory tract remains the primary focus of disease, with poor disease control leading to mediastinal extension and haematogenous dissemination that can involve any organ.13
The diagnosis of IA remains a challenge due to the absence of specific clinical manifestations, non-pathognomonic radiological findings and poor sensitivity of sputum cultures. In most cases, diagnosis is made by tissue isolation through invasive methods, as was the case in our patient. However, we felt attempting a less invasive approach namely image-guided fine-needle aspiration would have yielded the same results and should have been attempted first. Serological tests are adjuncts to support or exclude the diagnosis in the appropriate clinical context; however, they cannot be solely relied on for a definitive diagnosis.
Published literature highlights the poor, usually fatal outcome in patients with disease involving the mediastinum, despite initiation of antifungal therapy.14–16 This particularly holds truth in cases with delayed diagnosis leading to treatment delay and fatal outcomes. In this case, the patient continues to have a favourable outcome, with ongoing follow-up.
Treatment is often prolonged, with the duration of treatment determined empirically, depending on the extent of IA, the response to therapy and the immune status of the patient. Voriconazole is the first-line therapy for IA, with treatment duration depending on disease burden and host immunocompetence. The Infectious Diseases Society of America recommends 6 to 12 weeks of therapy for pulmonary aspergillosis.16 In immunosuppressed patients, therapy should be continued throughout the period of immunosuppression and until the resolution of lesions.16 Surgical treatment is reserved for patients who do not tolerate antifungal therapy or have residual localised but active lesions, despite adequate antifungal therapy.
This case highlights the importance of including the suspicion of IA in the differential diagnosis of a mediastinal mass presenting with signs of SVC syndrome irrespective of immune status, where TB and malignancy represent valid possibilities, as disease outcome is directly linked with early diagnosis and therapy.17 Early and timely treatment prevents future complications and death.
Learning points
Invasive aspergillosis (IA) is a rare but important consideration in immunocompetent patients presenting with signs of superior vena cava obstruction and a mediastinal mass.
Suspicion of IA in a patient, who does not respond to antibiotic or antituberculous therapy, is imperative in early diagnosis, allowing timely initiation of aggressive antifungal therapy and increasing the chances of a favourable outcome.
Imaging-guided percutaneous needle biopsy of mediastinal masses should be attempted first before reverting to a more invasive approach namely surgery.
References
Footnotes
Contributors The case report was conceptualised by JAK. YR reviewed patient records and examination along with literature research and writing the case report. Histopathology images were provided by AM. The final case report was approved by JAK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.