Article Text

Statistics from Altmetric.com
Description
A 15-month-old toddler presented to the emergency department (ED) with a history of fatigue, rhinitis and reduced oral intake. The medical history was remarkable for diarrhoea (Enterohaemorrhagic Escherichia coli (EHEC), Shiga toxin) positive haemolytic uremic syndrome (D+-HUS) 3 months ago with microangiopathic haemolytic anaemia, thrombocytopenia, renal failure and hypertension. When HUS was diagnosed, he had a blood pressure of 117/82 mm Hg, anuria over 18 hours and a platelet count of 110x109/L with fragmentocytes on blood film without evidence of complement dysfunction. The patient had come off dialysis after 1 month with persistent impaired renal function (peak creatinine 300 µmol/L, on discharge 205 µmol/L, estimated glomerular filtration rate (eGFR) 10 and 15 mL/min/1.73 m2, respectively). He was on regular amlodipine, calcitriol and sodium bicarbonate. Parents reported normal urine output. Clinical examination showed respiratory rate 62/min, no recessions, heart rate 154/min, blood pressure 122/98 mm Hg, pulse oximetry 100% and normal temperature. Lung auscultation revealed bilateral inferior crackles; heart auscultation was normal except for a louder second heart sound. Liver was not palpable and peripheral oedema was absent. Chest X-ray, blood count and serum chemistry were ordered.
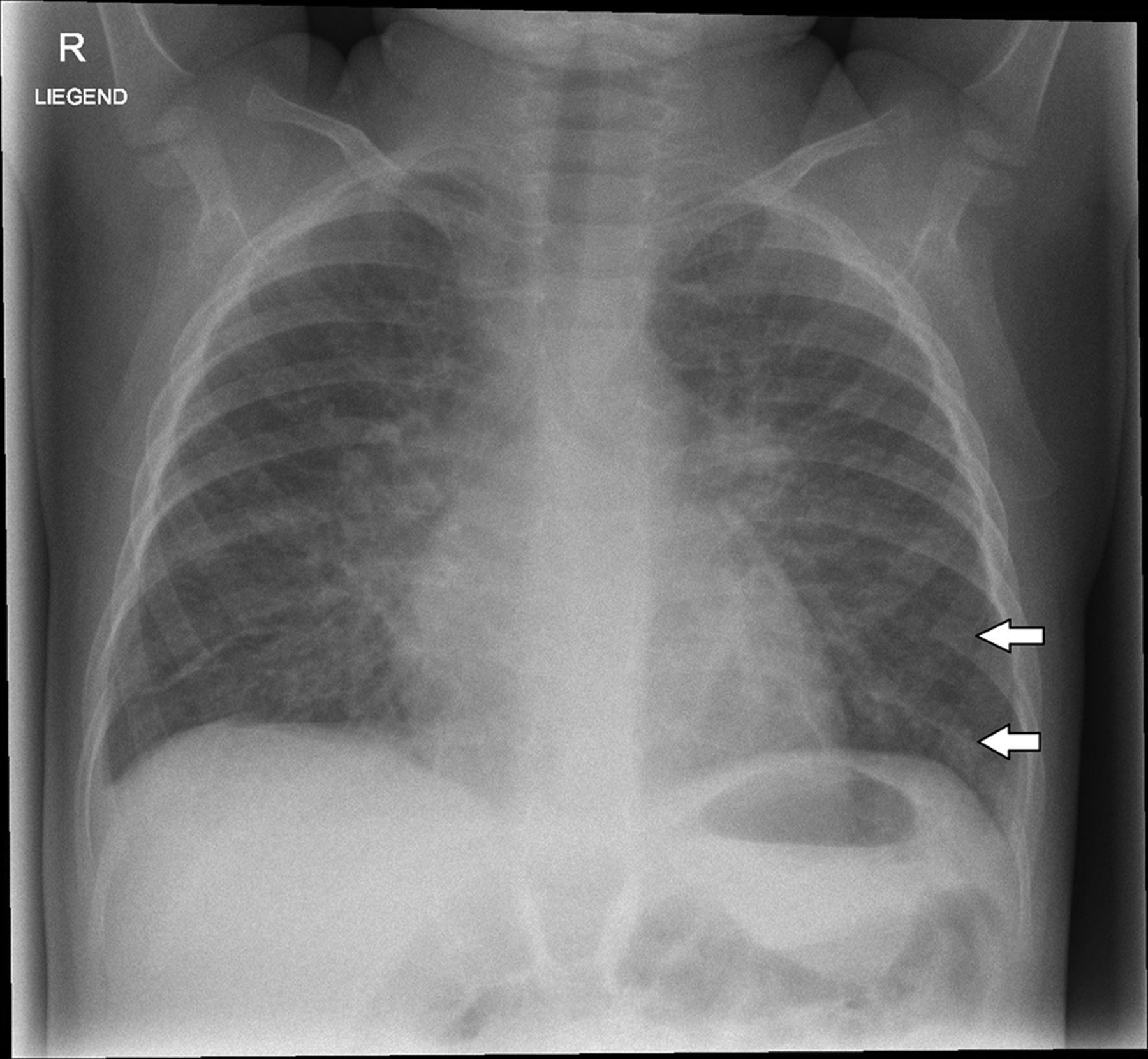
Imaging (supine) shows marked bilateral perihilar interstitial opacities, Kerley B lines on the left lateral inferior lung, no effusions and normal heart size (figure 1). Laboratory results indicated anaemia (haemoglobin 7 g/dL), elevated serum creatinine (259 µmol/L, normal <31, eGFR 12 mL/min/1.73 m2) and mild hyperkalaemia (5.6 mmol/L). The patient was diagnosed with pulmonary oedema due to fluid overload secondary to renal failure and transferred for ultrafiltration and dialysis to a tertiary centre.
{kind=link}
Chest X-ray supine, arrows indicate Kerley B lines.
Non-cardiogenic pulmonary oedema can occur secondary to near drowning, postintubation,1 trauma or transfusion, neurogenic pulmonary oedema,2 renal failure, drugs or inhaled toxins.3
HUS has an incidence of 1.9–2.9 cases per 100 000 children age <3 to 5 years in industrialised countries but is much higher in Latin America (10–17 cases per 100 000 children in Argentina).4 Pulmonary oedema can occur in a small fraction of hospitalised patients.5
Overall, pulmonary oedema is rare in the setting of a general paediatric ED.
Learning points
Pulmonary oedema in children presenting to the general paediatric emergency department is extremely rare.
Treatment of pulmonary oedema is supportive and based on the underlying cause.
Footnotes
Contributors LS and TJN were treating physicians and drafted the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.