Article Text

Statistics from Altmetric.com
Description
A 24-year-old female patient presented with acute-onset, vertex headache associated with photophobia, nausea and vomiting. Initially, the headache was mild (pain scale 4/10), but over the next 4–5 hours, the severity of the headache increased to pain scale of 8/10. She had a history of similar headaches of lesser intensity in the past. There was also a strong family history of migraine. Her mother and younger sister used to get similar headaches and got relieved with antimigraine medications. Exact details of her medication history were unavailable since the progression of severity of her headache was gradual. This was unlike thunderclap headache and, in high likelihood, another episode of migraine.
Her vitals were stable. Neurological examination, including funduscopy, was grossly normal
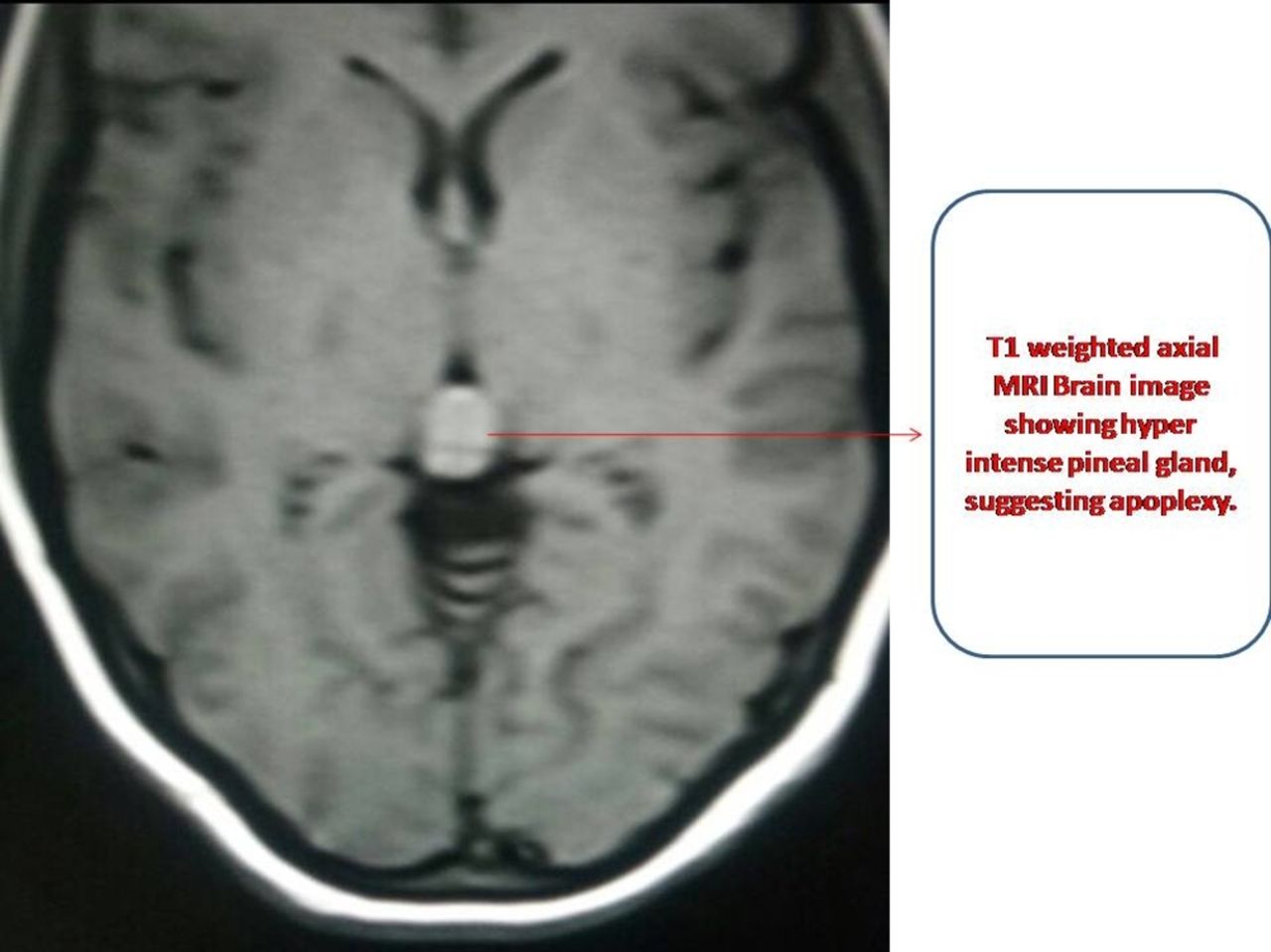
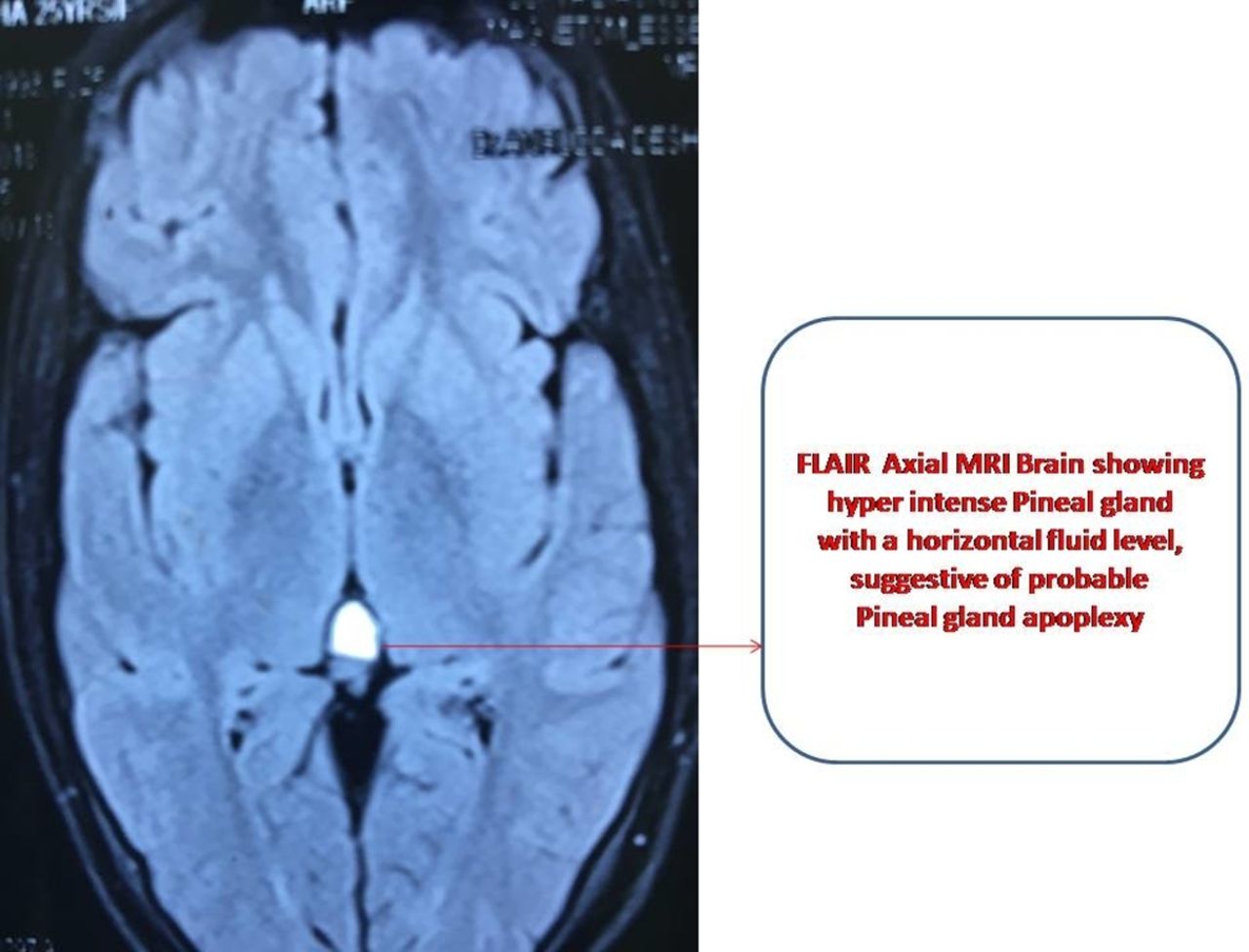
On radiological evaluation, the MRI brain showed T1-weighted hyperintense pineal gland, as seen on the axial view suggestive of intrapineal gland apoplexy (figure 1). The fluid–fluid interface is depicted by the horizontal sharp ‘cut-off’ on Fluid Attenuated Inversion Recovery (FLAIR) axial view suggestive of apoplexy, most probably in an intrapineal cyst (figure 2).

MRI brain showing T1-weighted hyperintense pineal gland, as seen on the axial view suggestive of intrapineal gland apoplexy.

Fluid–fluid interface depicted by the horizontal sharp ‘cut-off’ on FLAIR axial view, suggestive of apoplexy, most probably in an intrapineal cyst.
Similarly, the vertical sharp ‘cut-off’ on the posterior aspect of the pineal gland on T2-weighted sagittal view (figure 3) was a pointer towards recent haemorrhage probably inside a pineal cyst. Since the wall of the pineal cyst is thin, it may show heterogeneous enhancement in contrast MRI as shown in T1-weighted sagittal view (figure 4).

Fluid–fluid interface depicted by the vertical sharp ‘cut-off’ at posterior aspect on T2-weighted sagittal view, suggestive of apoplexy, most probably in an intrapineal cyst.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
T1-weighted sagittal view contrast scan suggestive of heterogeneous enhancement of wall of the pineal gland.
Apoplexy (meaning ‘a striking away’ in Greek) is bleeding within internal organs causing associated symptoms. Pineal apoplexy is rare medical condition. It refers to the acute neurological deterioration following bleeding in the pineal region, most commonly into a pineal cyst. It is mostly seen in women, aged between 20 and 30 years. The sensitivity of detection of cysts in the pineal gland depends on the size of the cyst. There is more likelihood of detection of cysts with a diameter of more than 5 mm by an MRI scan. Cysts <5 mm in diameter may not be picked up on the MRI.
The differential diagnosis in this case were
Cystic gliomas.
Pineal parenchymal tumours such as pinealocytomas.1
The pineal cysts are well-circumscribed, round-shaped lesions anatomically. MR imaging can identify intracystic haemorrhage by a characteristic fluid–fluid interface2 However, pinealocytomas may mimic cysts, and it is difficult to distinguish between the two on routine MRI scan.3
Learning points
Pineal gland apoplexy is a rare neurological condition and may mimic an episode of migraine headache.
MRI in pineal gland apoplexy identifies the intracystic haemorrhage by a characteristic fluid–fluid interface.
The differential diagnoses of pineal gland apoplexy are cystic gliomas and pineal parenchymal tumours such as pinealocytomas.
Footnotes
Contributors DKK and AD made substantial contributions to the conception and design of the work, acquisition, analysis and interpretation of the data. VK and SK were involved in drafting the work and revising it critically for important intellectual content. AD approved the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.