Article Text

Statistics from Altmetric.com
Description
A 17-year-old woman was admitted to the emergency department with a 3-day history of dyspnoea (New York Heart Association Class II) and typical pleuritic pain following a 1-week history of cough and fever. Pneumonia was diagnosed based on a chest X-ray (figure 1A), and amoxicillin–clavulanate treatment was initiated. After 48 hours, the patient developed hypotension and tachycardia. Given hypotension, ongoing fever and rising C reactive protein despite antibiotic treatment, she was referred to the intensive care unit. On admission, an echocardiography was performed. A circumferential pericardial effusion with 14 mm maximum diameter adjacent to the right ventricle was detected, without haemodynamic compromise at the time. Besides, left pleural effusion was evidenced. An ultrasound-guided thoracentesis was conducted. Pleural fluid testing revealed the following findings: white blood cells (WBC) count 11.109/Literwith 90% neutrophils, proteins 38 g/L, pH 7.36, glucose 6.3 mmol/L and lactate dehydrogenase (LDH) 492 IU/L. The culture exhibited no organism, and the cytology proved negative in terms of malignant cells.

Chest X-Ray (A) showing a right para-hilar mass (arrow). (B) Echocardiography showing pericardial effusion and external mass with compression of the left atrium (arrow).
The next day, another echocardiography was carried out, showing more extensive pericardial effusion with tamponade effect. Moreover, a mass compressing the left atrium was detected (figure 1B). Pericardiocentesis was performed and revealed an exudative fluid (protein 43 g/L) containing a WBC count of 10 660/mm3 with 90% neutrophils. Further routine testing revealed glucose 6.4 mmol/L and LDH 2397 IU/L. A Salmonella species (Salmonella Bredeney) was isolated in the pericardial fluid. Amoxicillin–clavulanate treatment was maintained in line with the antibiogram.
After review of multiple chest X-rays, a bronchogenic cyst was suspected based on the right parahilar opacity displayed on one such chest X-ray. The said opacity had already been observed on a previous image when the patient was 3 years old, in the course of treatment for pneumonia. Therefore, the diagnosis was confirmed via a CT scan determining a large mediastinal cystic mass measuring 75×53×63 mm and causing compression of the left atrium (figure 2A).
{kind=link}
{kind=link}
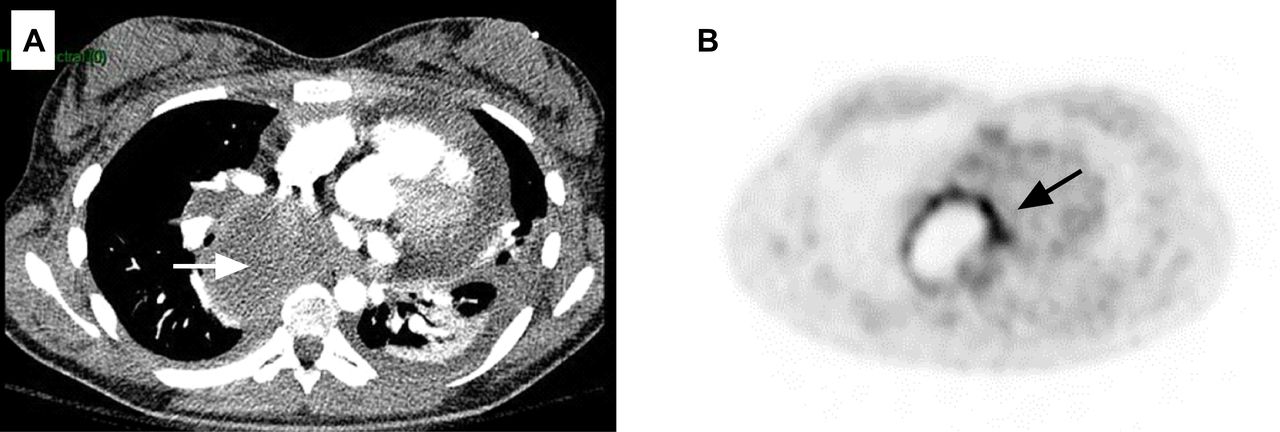
Axial view of chest computed tomography (A) showing 75x53x63mm mediastinal cystic mass (arrow) with left pleural effusion. (B) 18F-FDG- PET/CT revealing an uptake of 18F-FDG in a mediastinal cyst .
An 18F-FDG PET/CT scan was carried out revealing an FDG-avid lesion in the mediastinum (figure 2B), suggestive of an infection. The patient was referred to the thoracic surgeons straight away, as resection is recommended in cases of complicated bronchogenic cysts.1 2 She underwent a lateral thoracotomy and the cyst was excised. Histopathological examination confirmed the diagnosis of bronchogenic cyst. A purulent fluid filled the cavity, though the culture remained sterile. The patient fully recovered from this episode and was discharged on the 10th postoperative day.
Learning points
Bronchogenic cyst is a rare congenital malformation. It is discovered incidentally or when complications happens. Infection and compression are the main complications.
Patients with large pericardial effusion should be considered for bronchogenic cyst infection.
18F-FDG PET/CT can be used to prove a cyst infection.
Footnotes
Contributors J-BM is the first author and corresponding author of this manuscript. J-BM and C-ZD collected the clinical data. LG and OVC revised the manuscript. All authors contributed to the management of the patient and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.