Article Text

Statistics from Altmetric.com
Description
A full-term newborn boy was admitted to the high dependency unit at the age of 4 hours with signs of respiratory distress, tachypnoea and recession with low oxygen saturation. There was no perinatal history of concerns; delivery was normal and uneventful, but the mother was colonised with Group B streptococcus.
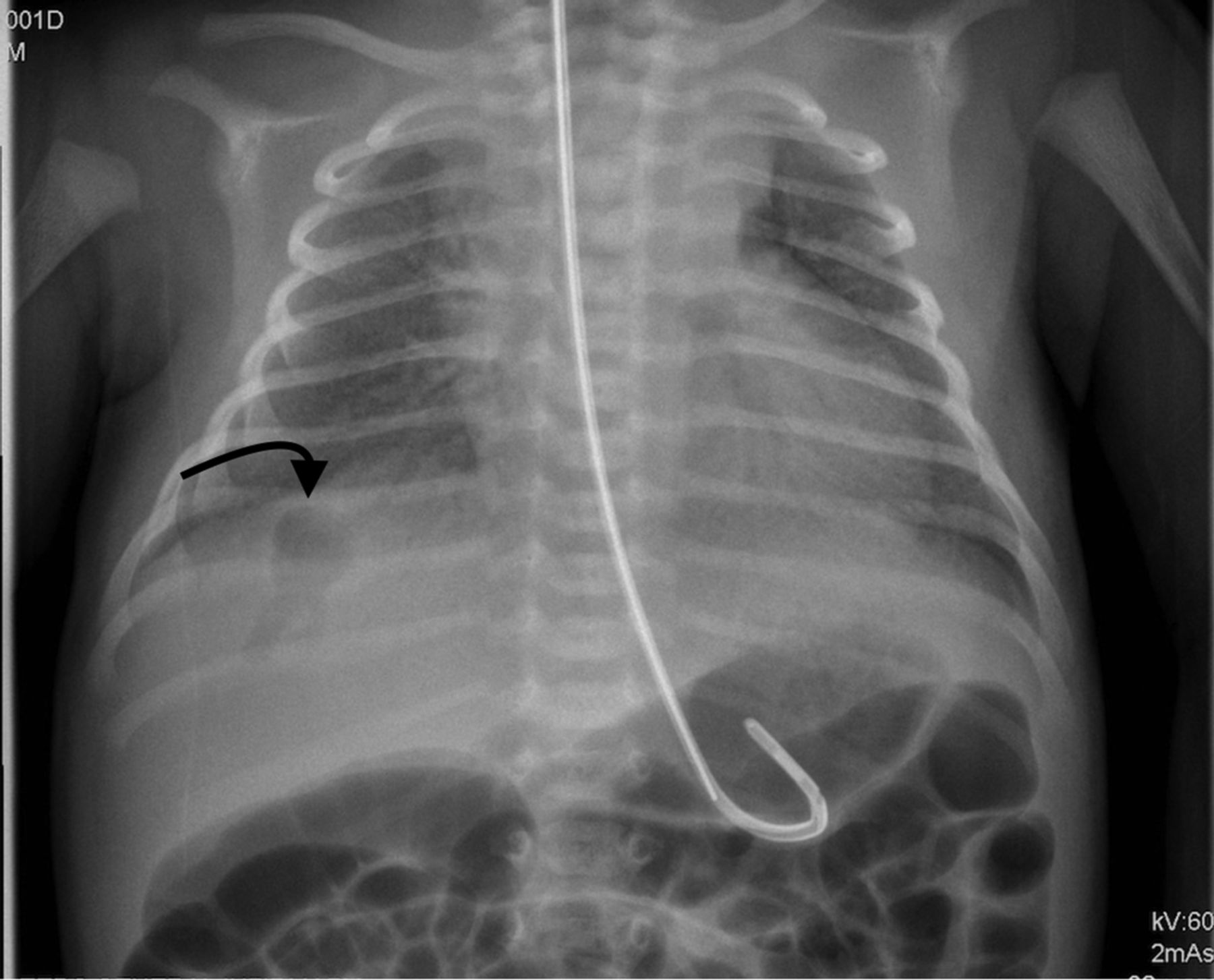
A plan was made on admission for a chest X-ray, a nasogastric tube (NGT) insertion and antibiotics. NGT was placed by a senior neonatal nurse without incident, followed by chest X-ray primarily looking for respiratory causes of the respiratory distress. This however revealed that the NGT was malposed into the right main bronchus (figure 1). There were no signs of choking or cough at the time of insertion. NGT was then pulled out and a new one reinserted in a satisfactory position and confirmed on a repeat chest X-ray (figure 2). A right-sided small and simple pneumothorax was noted on the repeat chest X-ray; conservative management continued with supplemental oxygen via nasal cannula. The baby in our case however continued to have tachypnoea and grunting, with worsening blood gases over the next few hours. A follow-up chest X-ray was therefore obtained and showed extensive right-sided tension pneumothorax (figure 3). An emergency needle aspiration was performed in preparation for intubation and chest drain insertion. The baby was haemodynamically stable and tolerated the intubation well, but he required two further chest drains over the subsequent few days due to recurrent tension pneumothorax. A bronchopleural fistula was highly suspected due to the air bubbling through the water seal of the drainage device in synchrony with the inspiratory phase during ventilation. A cardiothoracic surgical referral was averted as our baby made a good recovery afterwards. He stayed ventilated for a week and the last chest drain was successfully removed 2 days later. The baby was discharged home in good condition with neonatal follow-up appointment.

First X-ray with nasogastric tube in the right main bronchus.
Repeat chest X-ray: a small right-sided pneumothorax in the right lower zone.

{kind=link}
{kind=link}
{kind=link}
Right-sided tension pneumothorax.
NGT blind insertion is a standard procedure for hospitalised patients done by qualified medical staff. Changes in policies, staff training and development of vigilant institutional protocols for NGT insertion have led to a substantial decrease in the number of complications following malpositioned NGT. Yet there is still a rare but considerable risk of complications arising from this procedure for which medical practitioners need to be aware of.1 A high index of suspicion for any clinical changes should therefore be maintained and promptly investigated.2
Learning points
Practitioners should be aware of the possible pulmonary complications associated with blind nasogastric tube (NGT) placement.
A chest X-ray after the removal of a malpositioned NGT may be necessary to rule out lung injuries and bronchial complications.
Footnotes
Contributors OH has drafted the manuscript and LM was responsible for the final editing. OH and LM were involved in the clinical management of the patient and obtained the consent.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.