Article Text

Statistics from Altmetric.com
Description
A patient with neurofibromatosis 1 and childhood ventriculoperitoneal (VP) shunt insertion for hydrocephalus presented with 4 weeks of short-term and working memory impairment. Apart from right-hand tremor, he denied headache, visual changes, weakness and dyscoordination. A CT head showed a right-sided subdural lesion with 22 mm midline shift. The MRI head showed a right inferior-frontal enhancing mass suspicious of high-grade glioma and right extensively calcified subdural extra-axial collection, with mixed heterogeneous predominantly T1-hyperintense contents (figure 1A).
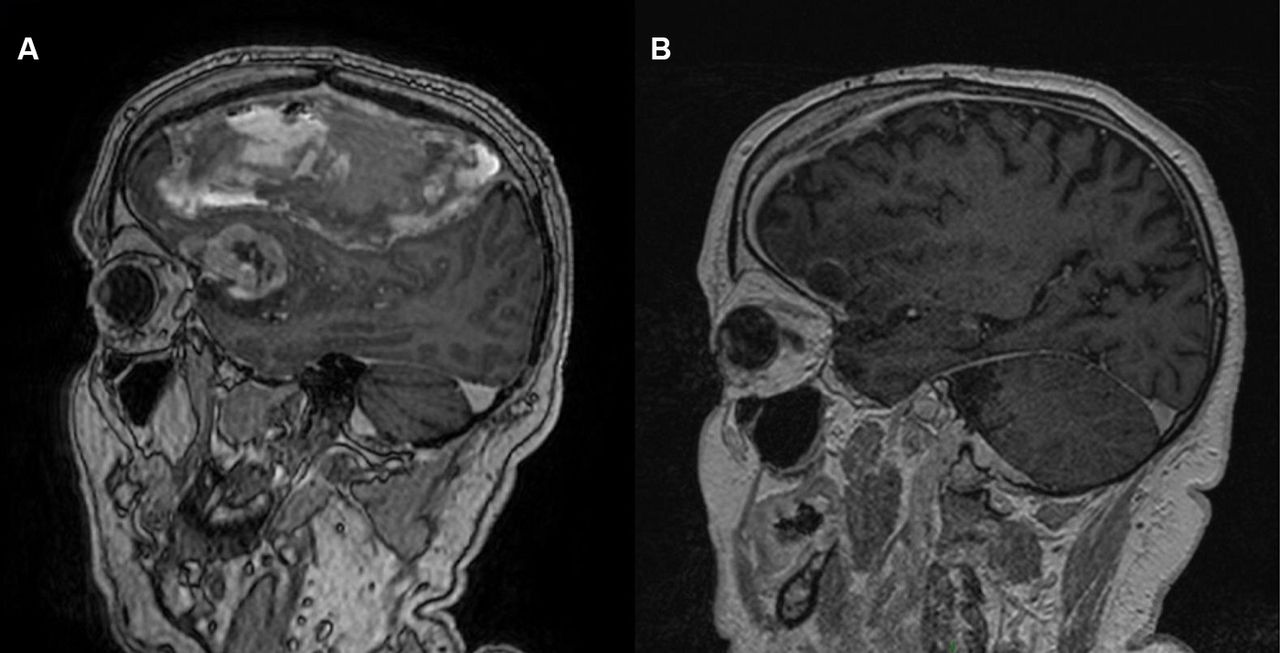
(A) Preoperative MRI shows a right inferior frontal mass suspicious of high-grade glioma and the extra-axial collection with mixed heterogeneous predominantly T1-hyperintense contents, and extensive calcification. (B) Postoperative MRI showing more than 90% debulking of the enhancing tumour (glioblastoma, WHO grade IV) and the right subdural evacuation.
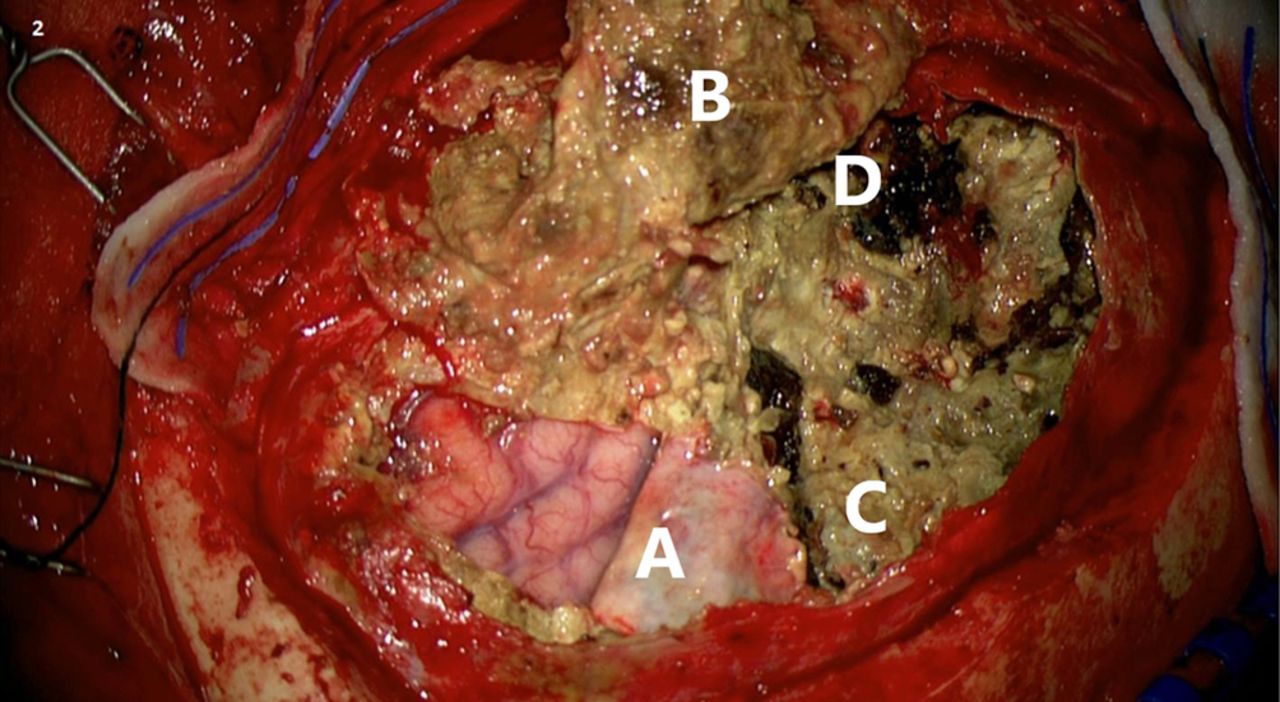
He underwent right fronto-temporo-parietal craniotomy with chronic calcified subdural haematoma evacuation, right frontal mass resection plus duraplasty (figure 2). A postoperative MRI showed more than 90% debulking of the enhancing tumour (glioblastoma, WHO grade IV) and successful subdural evacuation (figure 1B). He received concurrent chemoradiotherapy and was well 4 months after surgery. Unfortunately, he developed recurrent seizures 11 months after his operation and follow-up MRI showed increased enhancement suggesting tumour regrowth. Repeat MRI following further tumour debulking showed rapid glioblastoma progression and he was not for further surgical intervention. He passed away 12 months after his initial diagnosis.

{kind=link}
{kind=link}
Intraoperative image taken after the right fronto-temporal-parietal craniotomy, dural opening and partial evacuation of the chronic highly calcified multilayer subdural haematoma. It shows (A) the right inferior frontal lobe before tumour resection, (B) external subdural membrane, (C) internal subdural membrane and (D) the remaining chronic calcified subdural collection.
The glioma is likely responsible for his initial symptoms, but the coincidental calcified chronic subdural haematoma was striking. Non-traumatic subdural haematomas are recognised complications of VP shunt overdrainage, but calcification occurs in only 0.3%–2.7% of cases.1 2 If it were not for the symptoms caused by the glioma, the extensively calcified haematoma may not have been discovered 40 years after the insertion of his VP shunt.
Learning points
Overdrainage of ventriculo-peritoneal shunts may cause non-traumatic subdural haematomas.
Chronic subdural haematomas may be asymptomatic for many years.
Footnotes
Contributors ZW-YC was involved in drafting the manuscript and getting consent from the next of kin. PG was involved in conception, revising the manuscript and final approval of the version published. Both parties agree to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved. Both parties contributed to the revision of the original article after reviewer’s suggestions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.