Article Text

Statistics from Altmetric.com
Description
A man in his early 50s presented to the emergency department with complaints of abdominal pain and dark tarry stools. He reported 3/10 burning left upper quadrant abdominal pain that started 2 days before. The pain radiated to the epigastric region and the patient was unsure what exacerbates or relieves the pain. Starting around the same time, the patient had 8 to 10 black tarry stools daily, which were loose in consistency, which were coming out of his ostomy bag. Review of systems was positive for weakness, fatigue, nausea, abdominal pain and change in stools. The patient has a history of T4 caecal adenocarcinoma with metastasis to bladder diagnosed in 2014, for which he underwent right hemicolectomy, low anterior resection, radical cystectomy and colostomy with urostomy that was reversed 2 years later. He also underwent chemotherapy/radiation therapy with (FIFLORI) leucovorin calcium (folinic acid), fluorouracil and irinotecan hydrochloride. Vitals showed a temperature of 97.5°F, pulse 87 beats per minute, respiratory rate 16 breaths per minute and blood pressure 119/69 mm Hg. On physical examination, abdomen was soft, mildly distended, tender to palpation in the left upper quadrant and the left epigastric region, and no rebound or guarding was present. The colostomy was filled with black stool. Skin examination and ophthalmology examination were unremarkable. Urostomy had adequate output with no blood noted. Laboratory work-up was remarkable for acute normocytic anaemia with haemoglobin of 6.2 g/dL. The patient received continuous intravenous normal saline infusion and 1 U of packed red blood cell transfusion. Haemoglobin improved to 7.0 g/dL. General surgery team performed emergent oesophagogastroduodenoscopy, which showed a large ulcerated mass extending from the greater curvature that was actively bleeding (figure 1). A partial gastrectomy was performed, and a J tube was placed about 20 cm away from the ligament of Treitz. It was a large ulcerated mass within the stomach; histopathology showed (figures 2, 3 and 4) extensive involvement of the adjacent mucosa within the lamina propria that extended virtually to the serosal surface. There was widespread capillary lymphatic space involvement. The atypical cells were growing in solid sheets and appeared discohesive; cells were large with a high nuclear to cytoplasmic ratio and prominent large nucleoli. There were no identifiable glands. There was widespread mitotic activity and necrosis. There was no identifiable pigment formation, and there were areas of vascular invasion. Immunohistochemical stains showed strong staining with vimentin, melan A and SOX-10 (figure 5). The atypical cells of interest did not demonstrate staining with cytokeratin 7, cytokeratin 20, pan-keratin or CAM5.2. Molecular study was positive for p.V600E B-Raf proto-oncogene (BRAF) mutation. The above findings were suggestive of melanoma. PET/CT showed fludeoxyglucose-avid lymphadenopathy in the gastrohepatic ligament up to 1.1×1.4 cm with intense uptake standardised uptake value (SUV) 10.5 (figures 6 and 7). There was also interval enlargement of dominant lobular right middle lobe mass approximating 5.3 cm AP, SUV 15.1, biopsy of which showed an abscess with no malignant cells. Malignant melanoma is commonly known to manifest in the skin. Primary melanoma of the gastrointestinal tract is extremely uncommon, and it has been reported to arise from the mucosa of the oesophagus, anorectum and small bowel. To date, fewer than 15 cases of primary gastric melanoma have been reported in the literature.1 It can present with weight loss, upper gastrointestinal bleeding and anaemia. Positive immunohistochemical stains for S100 protein, Melan-A and HMB-45 antibodies are highly sensitive. Primary gastric melanoma is diagnosed when there are no concurrent lesions, the absence of a history of melanoma or prior removal of atypical melanocytic lesions from the skin or other organs. Prognosis is extremely poor due to the lag in diagnosis, aggressive nature of the tumour and easier metastasis due to the rich lymphatic and vascular supply of the gastrointestinal mucosa.2

Oesophagogastroduodenoscopy showing a large ulcerated mass extending from the greater curvature with active bleed.

H&E staining at low power (×4) showing gastric mucosal surface.

H&E staining at medium power.

H&E staining at high power.

Immunostaining positive for SOX-10.
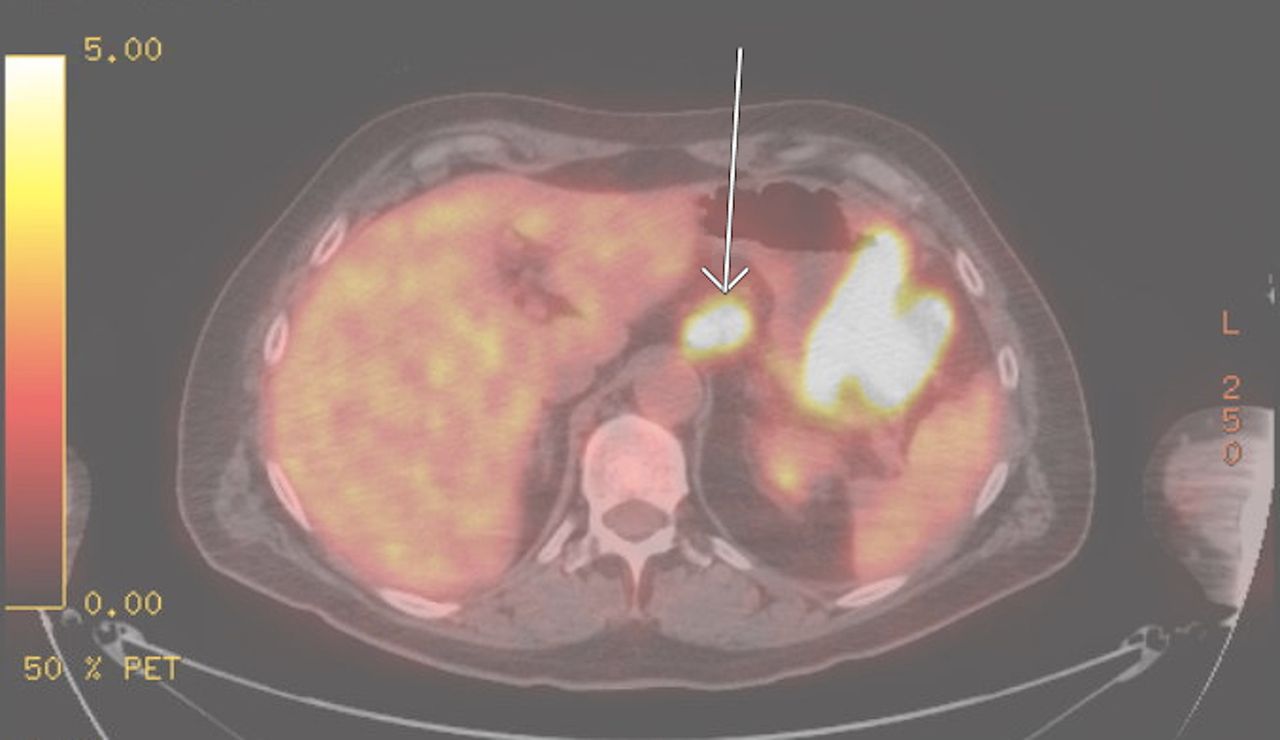
PET/CT (axial section) showing FDG-avid lymphadenopathy in the gastrohepatic ligament up to 1.1×1.4 cm with intense uptake SUV 10.5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PET/CT (coronal section) showing FDG-avid lymphadenopathy in the gastrohepatic ligament up to 1.1×1.4 cm with intense uptake SUV 10.5.
Learning points
Primary gastric melanoma is an extremely uncommon presentation of melanoma.
Amelanotic melanoma such as the one in this case can be missed in poorly differentiated tumours unless appropriate staining tests are performed.
Primary malignant melanoma of the stomach may be an underdiagnosed phenomenon.
Early detection and surgical intervention is critical for long-term cure, though overall prognosis is very poor.
Footnotes
Contributors MPR, DRN and SKK wrote the manuscript. MS revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.