Article Text

Statistics from Altmetric.com
Description
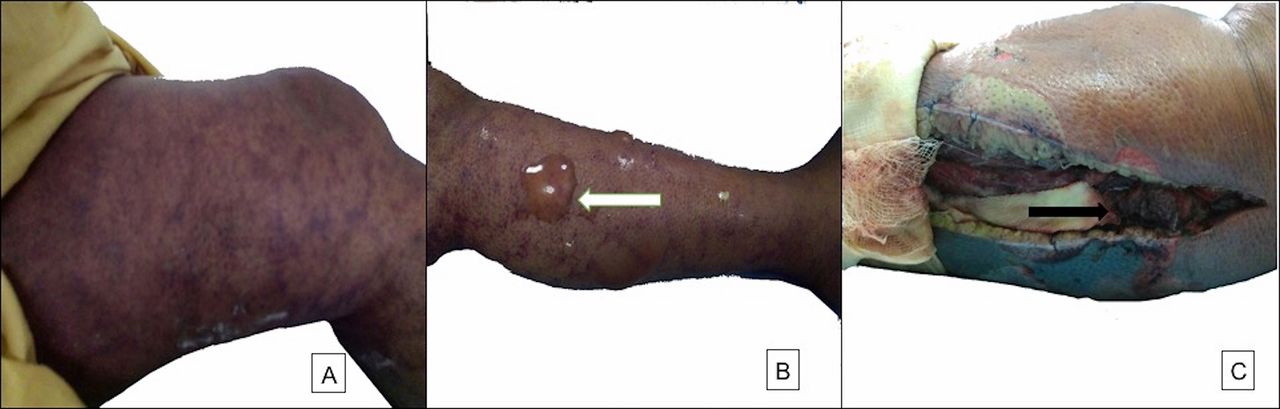
A 50-year-old woman, a known diabetic and hypertensive with poor compliance to treatment, presented with fever, dyspnoea and left-sided pleuritic chest pain for 15 days and left lower limb swelling worsening over the past 1 week. On examination, her vitals were stable, and she had significant left lower limb oedema extending up to the upper thigh with livedo reticularis (figure 1). The left lower limb pulses were not palpable. There was excruciating pain on light touch and passive flexion of the toes and ankle. Urgent arterial and venous Doppler sonography of the lower limbs revealed a left-sided iliofemoral venous thrombus. With the clinical diagnosis of acute compartment syndrome, urgent single incision four compartment fasciotomy was performed.
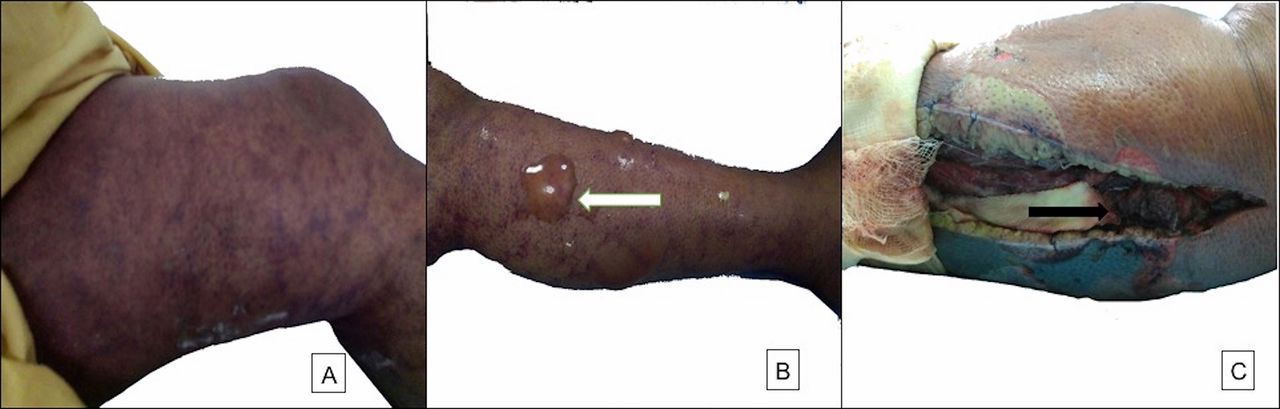
(A) Clinical examination at the time of admission showing lower limb oedema with livedo reticularis, (B) left lower leg livedo reticularis with superficial blistering (white arrow) and (C) postfasciotomy muscular necrosis (black arrow) which necessitated amputation of the limb.
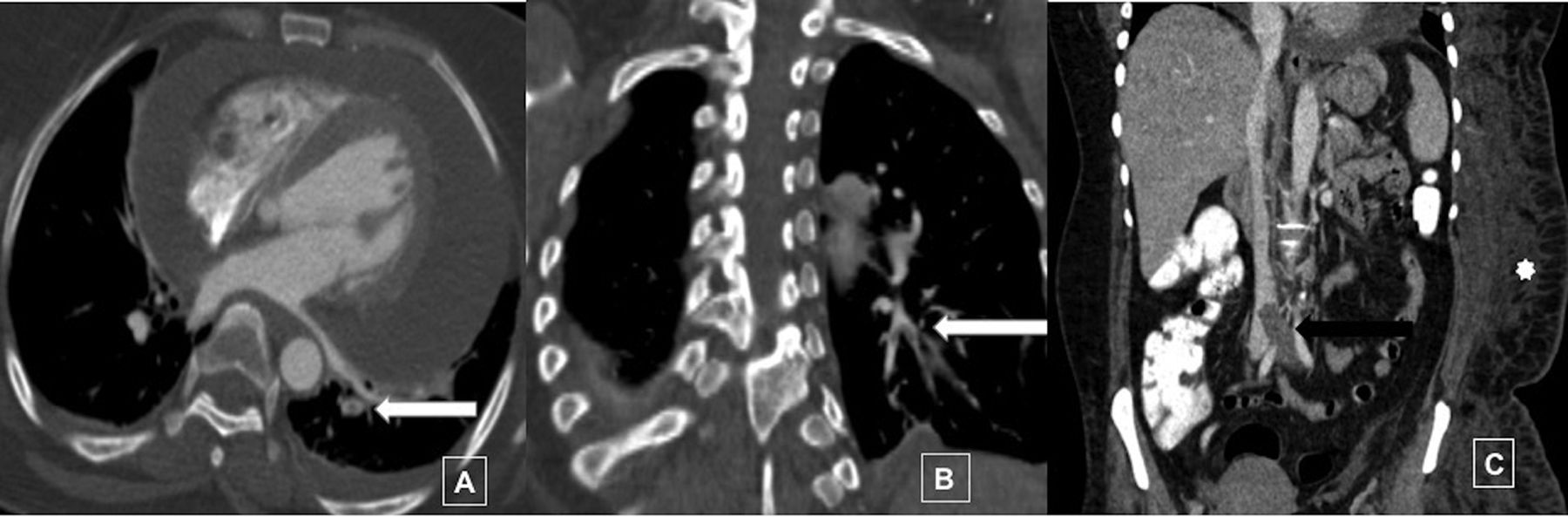
CT pulmonary angiogram demonstrated subsegmental pulmonary emboli in the territory of the left descending pulmonary artery (figure 2) and a moderate, predominantly posterior pericardial effusion. There was no evidence of either cardiac tamponade or right ventricular strain on bedside echocardiography. CT abdomen revealed a large deep venous thrombosis (DVT) extending from the left-sided calf veins to the infrarenal inferior vena cava with submassive pulmonary embolism and moderate pericardial effusion (figure 2). These findings were suggestive of phlegmasia cerulea dolens (PCD) with pulmonary embolism. The patient was initiated on anticoagulation with unfractionated heparin and supportive care such as lower limb elevation and analgesics. Her eventual work-up for malignancy and blood cultures were negative. Despite 12 hours of anticoagulation, her pain and swelling did not subside.
{kind=link}
{kind=link}
CT pulmonary angiography (A) axial and (B) coronal reconstruction showing filling defect in the segmental branches of the descending left pulmonary artery (white arrow). (C) Coronal contrast-enhanced CT abdomen showing hypodense thrombus filling the common iliac vein extending into the distal inferior vena cava (IVC) (black arrow). The proximal IVC shows normal contrast opacification. Also note the extensive subcutaneous soft tissue thickening along the left side (*).
Lack of response, limb-threatening DVT and ischaemic pain warranted aggressive management. As per institute’s protocol, catheter-directed thrombolysis (CDT) was offered. The patient did not consent for the procedure owing to the explained high risk of intracranial bleed. Despite therapy, the pain persisted and the patient developed gangrene of the lower limb and underwent below knee amputation. On the third postoperative day, she developed cough with dyspnoea which progressed to septic shock. Despite broad-spectrum antibiotics, she succumbed to her illness on the seventh postoperative day.
PCD is a poorly understood, fulminant, limb-threatening and life-threatening condition which is caused by acute massive venous thrombosis.1 It is characterised by the triad of pain, oedema and bluish discolouration of the limb.2 Due to its rarity, there is no consensus regarding its management though anticoagulation, catheter-directed thrombolysis and mechanical thrombectomy form the mainstay of management.1 Acute compartment syndrome characterised by ongoing tissue hypoperfusion due to raised intracompartmental pressure is a rare complication of DVT and has been previously described in PCD.2
High index of suspicion is of utmost value in management of acute compartment syndrome ACS as ischaemia for as little as 8 hours can lead to irreversible damage of the limb. Fasciotomy is the treatment of choice for ACS though the ideal duration and role of prophylactic fasciotomy is still not well understood.3
Patient’s perspective
Written by the husband
It was shocking as well as frightening how a fever led to so many complications. We had never imagined such terrible horror awaits us. Her initial distress was worrisome, her lower limb pain was the most terrible. Despite all the measures like cutting her leg open she couldn’t get relief. When we were told her leg blood vessels have clots we thought it might be like some boil we get on our face never to have thought it was so long and might take her away from us.
I thank the doctors for spreading awareness about her case. I wish nobody suffers from such a disease and if some one does they get cured of it.
Learning points
Phlegmasia cerulea dolens is an acute limb-threatening venous thrombosis which requires prompt and aggressive management.
High index of suspicion must be kept for the development of acute compartment syndrome in such patients.
Early fasciotomy is an effective way of limb salvage for these patients.
Acknowledgments
Dr Surabhi Vyas, Department of Radiology for the CT images and description.
Footnotes
Contributors ADS and NM were the residents involved in the management of the case. AR was the consultant in charge of the case. RS is the head of the department and was directly involved in supervision , crucial management and decision-making. Photographs were collected by ADS. ADS and NM were involved in editing. All the four authors were involved in writing and finalising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.