Article Text

Summary
A 58-year-old agricultural worker from a remote Western province farming community in Saudi Arabia presented with a 2-year history of right plantar foot soft tissue mass. According to the patient, the swelling had gradually increased in size over a few years, but it was painless and thus had not restricted him from continuing to farm until the lesion started to affect mobility. An MRI, microbiology and histopathology reported a rare infectious agent—Actinomyces spp, otherwise referred to as Madura foot. Three-dimensional CT aided in a preoperative surgical plan which included mass excision/debulking for this challenging lesion. Full eradication was not possible, and the patient required prolonged anti-infective therapy (>6 months) along with close surveillance to map resolution of infective symptoms.
- endocrinology
- diabetes
- infectious disease
- tropical medicine (infectious disease)
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Background
Actinomycosis is a rare infectious disease that often presents as a chronic pathology either due to misdiagnosis or patients unwilling to seek speedy medical advice. Primary Actinomyces spp, infection of the lower extremity is very uncommon because of the endogenous habitat of the organism. It can cause destructive changes to both the skin and soft tissue and progress deeper to involve bone. The cases can be complex to both diagnose and manage, particularly where tumefaction exists. Surgical planning is required to ensure the most effective excision of the mass is achieved and imaging modalities such as three-dimensional (3D) CT may aid in the preoperative planning phase. Overall, the aim of a surgical approach is to lower the prolonged requirement for anti-infective therapy.
Mycetoma is commonly observed in tropical/subtropical environments where it favours geographical areas that are dry and arid, such as Sudan, Nigeria, Ethiopia and Saudi Arabia.1 The ability for easy migration in the 20th century makes it possible for this pathology to present to clinicians around the globe. Documented cases have already been reported from the USA, Mexico and the UK.
Case presentation
A 58-year-old man presented with a 2-year history of soft tissue swelling (approximately 9 cm in diameter) on the plantar aspect of his left foot (figure 1). The patient was a farmer who worked in a remote area in the Western province of Saudi Arabia. According to the patient, the swelling had gradually increased in size over a few years, but it was painless and thus had not restricted him from continuing to farm his land for the best part prior to presenting for an opinion. As the sole income earner for his family, the reason for now seeking medical advice was owing to the inability to continue farming his land due to the large size of the lesion restricting him from mobilising normally and not being able to wear any types of shoes/sandals. The patient was a poor historian regarding his medical history and rarely sought medical advice. Further questioning, however, revealed that he had type 2 diabetes (no known duration) and penicillin allergy. The patient could not recall a ‘starting event’ or episode of trauma associated to the mass, and his estimation of the duration of the mass at 2 years was speculative at best.

(A) A large soft tissue mass on the plantar aspect of the foot from anterior to posterior. (B) A lateral view of the soft tissue mass demonstrates the extent of the growth which limited the patient’s mobility.
On examination of the mass, it was painless, firm, with no fluctuance. The patient was afebrile with no clinical signs of infection (erythema, heat, purulence).2 There were no lymphatic streaks or palpable inguinal adenopathy. The mass extended from the plantar aspect of the foot, extending dorsally between the third and fourth toe webspaces. On the plantar aspect of the mass were areas of small crusted lesions that sporadically discharged fliud were reported by the patient.
A diabetes foot screen was performed, and this identified that peripheral pulses were present and handheld Doppler (ArjoHuntleigh Dopplex SD2 bi-directional Doppler with 8MHz probe) identified biphasic, strong waveforms. A neurological examination using the Modified Neuropathic Disability Score (10/10) revealed loss of protective sensation.3 This finding likely explained the lack of pain associated to the mass and ability to continue weight bearing pain-free for an extended period of time.
Investigations
Routine blood tests were performed with the majority of chemistry within normal ranges. There were, however, elevated inflammatory markers (erythrocyte sedimentation rate 50 mm/hour, C-reactive protein 21 mg/L), suboptimal glycaemic control (NGSP haemoglobin (Hb) A1c=9.2%, IFCC HbA1c=217.6, eAG mg/dL=77 mmol/L) and reduced renal function/moderate CKD stage 3b (eGFR 50 mL/min).
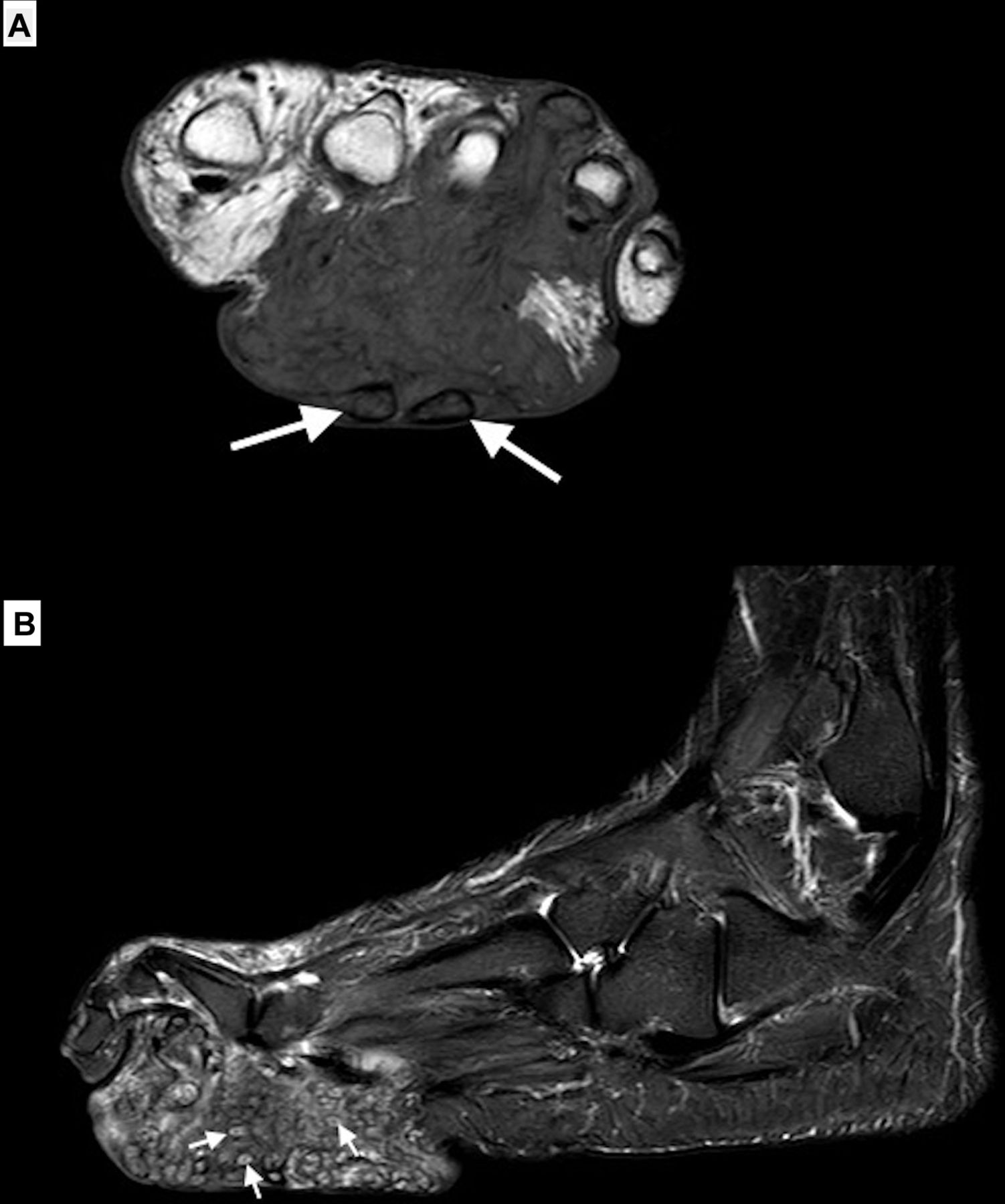
MRI on T2-weighted, Short-T Inversion-Recovery (STIR) and T1-weighted fat-saturated contrast-enhanced images reported a nodular infiltrative soft tissue lesion but sparring of osseous structures. The presence of ‘dot-in-circle’ sign4 was demonstrated with tiny hypointense foci within hyperintense spherical lesions in keeping with actinomycetoma (figure 2).

(A) MRI T2-weighted coronal image and (B) sagittal plane image show inflammatory changes with multiple soft tissue small hyperintense lesions showing ‘dot-in-circle’ sign.
To assist in the surgical planning of this complex case, a 3D CT with contrast was arranged. A nodular infiltrative mass was demonstrated measuring 9 cm in the anteroposterior dimension x 7 cm in the craniocaudal dimension and 5.6 cm in the transverse dimension. The mass extended from the plantar surface to the dorsum, involving the interdigital areas 2–4. The mass encased the digital arteries and the digital nerves as well (figure 3).

Three-dimensional CT illustrating the extent of the infiltrative mass.
No bone biopsy was obtained due to the negative reports of osseous involvement from both MRI and CT. A tissue punch biopsy at the plantar aspect of the lesion was sent for analysis; matrix-assisted laser desorption ionisation time-of-flight (MALDI-TOF), conventional microbiology, culture and sensitivity, and histopathology with requests to look for mycetoma (fungal/bacterial), acid-fast bacillus (AFB) and Nocardia Fite stain. No mycobacteria or fungal elements were detected through conventional culture or MALDI-TOF, and no AFB or Nocardia Fite stain was seen. A Gram-stained smear of the tissue specimen demonstrated the presence of branched, Gram-positive filamentous rods consistent with Actinomyces spp. Tissue samples sent for histopathology illustrated morphology consistent with filamentous Actinomyces spp (figure 4).

(A) H&E stain demonstrating sulfur granules (arrow a) from a sinus/abscess in the plantar foot (arrow b). The granules are composed of branched, Gram-positive filaments of Actinomyces. Surrounding the abscess are inflammatory infiltration of neutrophils (arrow c). (original magnification ×300). (B) Gomori methenamine-silver stain showing the presence of numerous thin filamentous mycelia radiating outwards.
Differential diagnosis
Malignant neoplasm.
Eumycetoma.
Treatment
The patient was admitted to hospital, where, after consultation with infectious diseases (in keeping with good antimicrobial stewardship practices) he was started on parenteral ceftriaxone 2 g two times a day (antimicrobial choice in the presence of a penicillin allergy). A surgical approach was undertaken with the aim of removing as much soft tissue mass as possible to help restore mobility, aid in the ability to wear protective footwear and attempt to eradicate the bacterial infection.
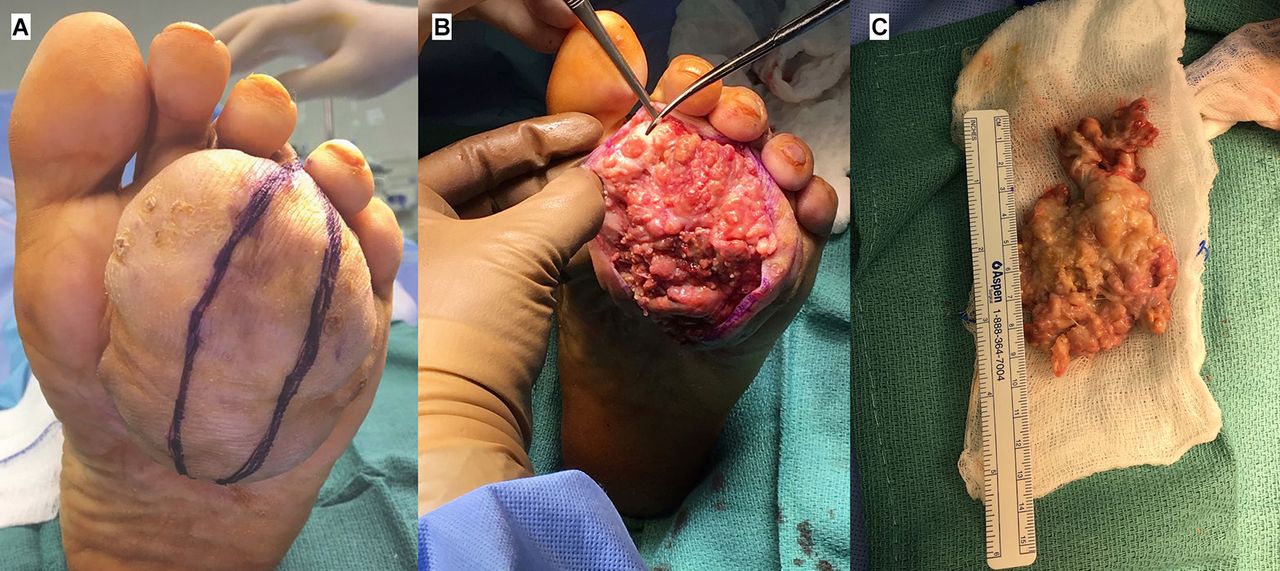
The patient received a regional block to the lower extremity and an elliptical incision was made on the plantar aspect centrally to the mass. A 9 cm x 6 cm firm nodular mass was excised from the plantar aspect in addition to excision of as much tissue interdigitally (figure 5). Due to extensive deep dermal invasion, the surgical procedure considered was debulking rather than eradication.5 Further intraoperative deep tissue specimens were sent for microbiology and histopathology, with both again confirming primary diagnosis of Actinomyces spp. Sensitivity patterns from the culture of intraoperative tissue samples confirmed the isolated strain of Actinomyces sp was sensitive to penicillin. The patient was started on doxycycline 100 mg tablet (due to a penicillin allergy) taken orally every 12 hours for a period of 6–12 months. This was necessary because full eradication of all infected tissues was not possible.
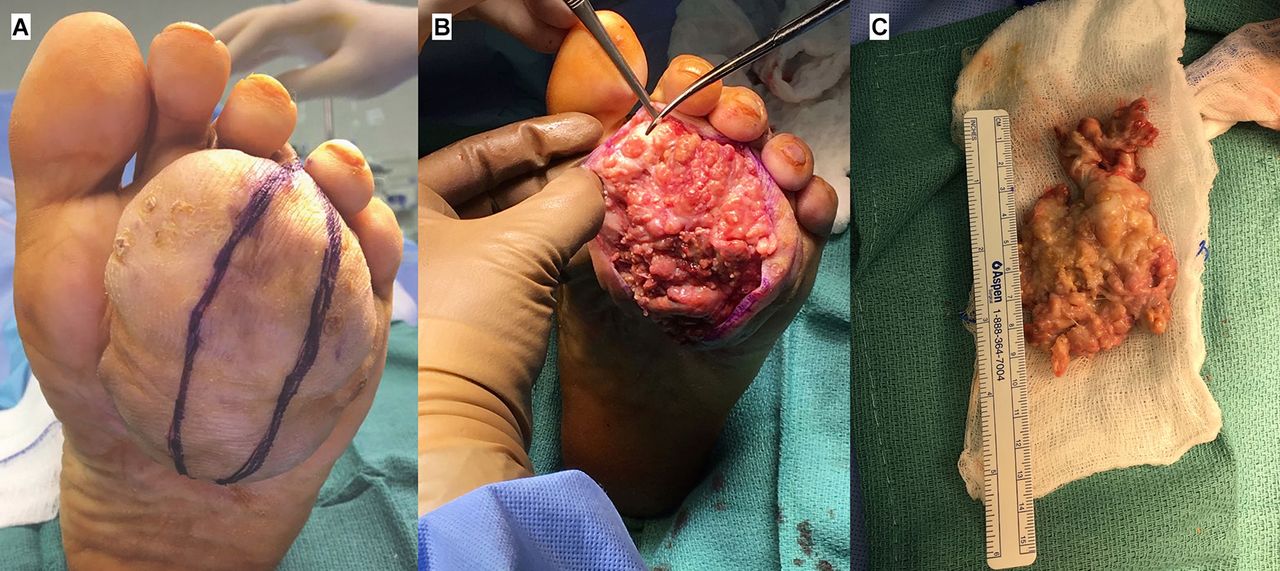
(A) The surgical approach using an elliptical incision to gain adequate access to the mass, while ensuring good approximation of the wound edges for reduced scarring on the plantar aspect of a weight-bearing area. (B) The extent of the nodular infiltrative mass. (C) Excision of the bulk mass.
Following a 10-day admission, the patient was discharged back to the care of a local healthcare provider near his remote farmlands with a requirement to attend for monthly checks in order to address glycaemic control, regular blood test for his renal profile and assessment for down-trending inflammatory markers.
Outcome and follow-up
An extensive follow-up period is required for most patients because postoperative recurrence of mycetoma even after adequate medical and surgical treatment is common and a serious problem.6 At 1 month postoperatively, there was complete healing of the incision sites (figure 6). The patient had returned to farming and was wearing protective footwear. He was also attending his local healthcare provider for monitoring of the aforementioned comorbid variables. An MRI at 3 months showed significant improvement to the soft tissue envelope, and the patient was continuing to adhere to his antibiotic regimen with no adverse effects. At his last follow-up, 6 months from surgery, he remains well with no recurrence of the mass clinically. The patient is scheduled for further MRI scans yearly at 12 months and 24 months following surgery and will remain under surveillance at 6 monthly intervals.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Three-month follow-up shows healed suture lines with a reduction in the bulk of the soft tissue mass.
Discussion
Mycetoma describes a rare pathology caused by either a true fungi (eumycetoma) or by filamentous bacteria (Actinomycetes species).7 It is predominantly a disease of tropical or subtropical countries whereby eumycetoma are commonly associated with soil or plants. Actinomyces species are Gram-positive facultative anaerobic bacteria that normally colonise the human mouth, digestive and genital tracts. While it is necessary for anti-infective treatment purposes to distinguish between the infectious agent responsible for mycetoma, the clinical manifestations of either microorganism are similar. The pathology often presents as a chronic infection of the skin and subcutaneous tissues in the presence (or sometimes absence) of tumefaction, discharging sinuses with the presence of black, yellow or white grains (hyphae). Differential diagnosis of actinomycosis are malignant neoplasia, tuberculosis or nocardiosis because it spreads continuously and progressively.8
The pathogenesis for mycetoma is dependent on the infective agent. In patients who develop mycetoma caused by fungi, it most often occurs after inoculation by means of trauma, with some patients having no recollection of an instigating factor. It is typically linked to agricultural occupations or exposure in those living in agricultural environments such as farm workers. Previous reports have identified causality in cases related to inoculation from standing on a splinter or thorn,1 allowing entry of the soil saprophyte. In the case of actinomycosis, the infecting bacterial organism is commonly associated with the mouth or gut. Infection may therefore develop with tooth decay, dental surgery, a burst appendix or inhaling liquid or food contaminated with the bacteria.
In this case report, our patient was a farm worker, yet he developed the bacterial form of mycetoma commonly associated with human microflora. A compounding factor in this case may have been the patients underlying diabetes with loss of protective sensation. Traumatic foot wounds are common in this cohort, and this may have precipitated entry of this uncommon bacteria.
Due to its often-slow progression, many cases present as chronic pathologies as they initially cause no impairment to function. However, as the mycetoma infection progresses, invasion into deeper structures accompanied by increasing visual or functional impairment often initiates patients to seek medical advice. Since phenotypic identification of the causative bacteria/fungi is often difficult using conventional microbiology, tissue or bone biopsies are better evaluated using either MALDI-TOF or molecular (DNA sequencing) methods if accessible. In addition, histopathology may augment these techniques.8 Imaging modalities such as MRI or CT often augment both the clinical picture and microbiology work-ups. Importantly, they may help to ascertain the extent of invasion, involvement with other tissue, nervous and vasculature structures in readiness for preoperative planning. Full excision of any infected tissues may not be possible as demonstrated in this case study, yet even in the absence of surgery, anti-infective regimens are often prolonged because of the tendency of Actinomyces spp or eumycetoma to recur.
A treatment algorithm for actinomycosis has been described by Schneider and Moos.9 For extensive lesions/soft tissue mass/abscess, surgical excision is required. Eradication or debulking will assist in the reduced requirement for prolonged anti-infective treatments. The first-line agents of choice for Actinomyces are penicillin or amoxicillin. Primary options include benzylpenicillin 6–12 g/day intravenously given in divided doses every 4–6 hours for 4–6 weeks, followed by phenoxymethylpenicillin 2–4 g/day orally given in 4–6 divided doses for 3–6 months after cessation of intravenous therapy. Alternatively, ampicillin 50 mg/kg/day intravenously given in divided doses every 8 hours for 4–6 weeks, followed by amoxicillin 500 mg orally three times daily for 3–6 months. Where penicillin allergies exist, ceftriaxone, clindamycin, erythromycin or doxycycline can be used.10 Eumycetoma (fungal) infections require similar long-duration regimens with antifungal therapies that include itraconazole, voriconazole or posaconazole.11 Regardless of the anti-infective, practices should be in keeping with good antimicrobial stewardship, hence infectious disease physicians form an integral team member.
Learning points
Actinomyces bacterial infections have been reported in body regions that include cervicofacial, abdominopelvic and pulmonothoracic. However, here we show its presentation as the cause of Madura foot.
Management requires aggressive control of any soft tissue invasive mass, often followed by prolonged antibiotic therapy.
Surveillance is required due to the tendency of actinomycosis to recur. Repeated clinical assessment, imaging and/or biopsy may prove useful in tracking this chronic and persistent pathology.
For mass lesions, surgical debulking may improve quality of life and aid in ‘source control’ for greater antibiotic therapy success.
Footnotes
Contributors The submitted case report has been undertaken solely by AAG. AAG was the consulting physician, requested all diagnostic tests and performed the surgery.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.