Article Text

Statistics from Altmetric.com
Description
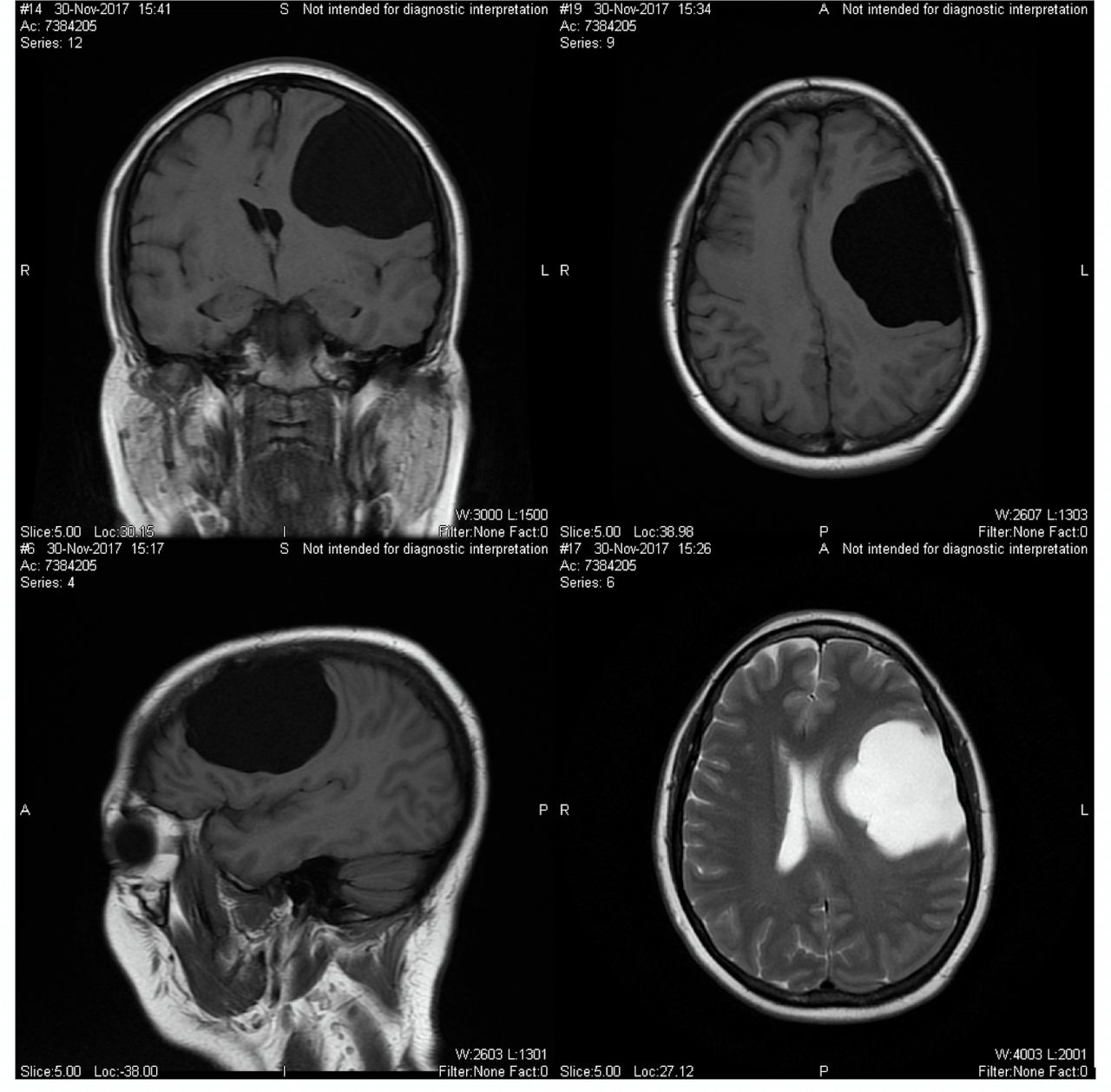
A 56-year-old woman with no significant medical history was brought for evaluation of difficulty with speaking for 1 month. Family reported patient having short-term and long-term memory impairment and gradual cognitive decline over a course of 2 years. Her mother had Alzheimer’s dementia in her 60s and the patient attributed her symptoms to Alzheimer’s and did not seek medical attention until she developed word finding difficulty. On neurological examination, she had expressive aphasia and scored 20 on Mini-mental state examination (MMSE). Laboratory work-up showed normal haemogram, metabolic panel, thyroid function tests, vitamin B12 and folic acid levels and a negative rapid plasma reagin (RPR) test. MRI showed a giant left cerebral hemisphere arachnoid cyst with 11 mm midline shift to the right (figure 1). She underwent stereotactic craniotomy with microsurgical excision of the arachnoid cyst. Postoperative hospital course was complicated by generalised tonic–clonic seizure, controlled with antiepileptic medications. On 6-week follow-up, patient had resolution of expressive aphasia and mild improvement in her cognitive function.

{kind=link}
T1-weighted coronal (left upper), sagittal (right upper) and axial (left lower) images on MRI brain without contrast showing left parietal lobe arachnoid cyst measuring 6.7 cm × 5.3 cm with 11 mm midline shift to the right. T2- weighted sagittal (right lower) images of the brain showing isointensity with cerebrospinal fluid. There is the homogeneity of the lesion, lack of perceptible wall and lack of internal complexity which are suggestive of an arachnoid cyst.
Arachnoid cysts are cerebrospinal fluid-filled sacs located between brain or spinal cord and arachnoid membrane.1 Primary arachnoid cysts are more common and congenital in origin whereas secondary arachnoid cyst can develop as a complication of brain surgery, head injury, tumour or meningitis.1 These comprises about 1% of all intracranial mass with approximately 50%–60% occurring in the middle cranial fossa.1 2 Males are four times more likely to have arachnoid cysts than females.2 Elderly patients with arachnoid cyst usually present with headache, nausea and vomiting, vertigo, gait disturbance and dementia, mimicking chronic subdural haematoma and normal pressure hydrocephalus.2 3 MRI is the diagnostic study of choice in the detection of intracranial arachnoid cysts. Neurosurgical procedures like craniotomy with cyst wall excision, stereotactic cyst aspiration, shunting of cystic fluid to the peritoneal cavity and endoscopic fenestration of cysts to the subarachnoid space or the ventricles can be used to decompress the cyst.2
Learning points
Thorough work-up is of utmost importance to rule out reversible causes of dementia, even in cases with very strong family history of Alzheimer’s dementia.
Arachnoid cysts, although more common in younger patients, should always be considered as a differential diagnosis for a patient being evaluated for neurological symptoms.
Removal of arachnoid cyst with neurosurgical interventions can significantly improve neurological symptoms.
Footnotes
Contributors All authors were directly involved in the care of the patient and contributing to this article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.